So far, two months and 6000 views. What can I say? Thank you! The article with greater interest has been the one on body posture (read it here), about the importance of body alignment and how craniofacial development affects total body posture. The second most popular was the article on hair loss (available here), where the current androgenetic theory is questioned and a new model has been proposed. Let us clarify some concepts expressed in there.
Current theories see the dihydrotestosterone (DHT) hormone as the main responsible for hair loss. As the name suggests, there are two supposed causes for androgenetic alopecia: the action of hormones (androgens) and action derived from genetic.
The theory started to arise after observations made on Eunuchs (i.e. men who have been castrated). Already in 400 BCE, Hippocrates noticed that Eunuchs do not become bald [1], with formal conclusions made by James B. Hamilton between 40s and 60s: eunuchoid and prepubertally castrated men fails to achieve sexual maturation and show complete retention of head hair [2]. Baldness can then be induced by following administration of male hormone substances to sexually immature men who otherwise would not have become bald [3]. In 1974, a study has generally observed a higher formation of 5α-reduced metabolites and 17-ketosteroid metabolites at all sites of the scalp of bald men as compared to hair obtained from the corresponding sites of women and nonbalding men [4]. So, from here it has been assumed the importance of DHT in baldness.
However, many arguments are against the role of DHT as primary cause in hair loss:
DHT stimulates the production of pigmented terminal hair in many areas after puberty, including pubic and axillary hair in both sexes and beard growth in men. But both beard growth and balding can occur on the same person demonstrating a paradox [5,6].
Serum androgen concentrations in men with a disposition to balding is lower than in men with no reduction of scalp hair [7].
The prevalence of Male Pattern Baldness increases with age [8]. However, serum testosterone production declines with aging [9], together with lower serum DHT [10].
Female androgenetic alopecia can develop in the absence of detectable levels of circulating androgens or other signs of postpubertal androgenization, showing that this pattern of hair loss is not necessarily androgen dependent [11]. Not only, female patients with androgen deficiency reports hair regrowth on testosterone therapy [12].
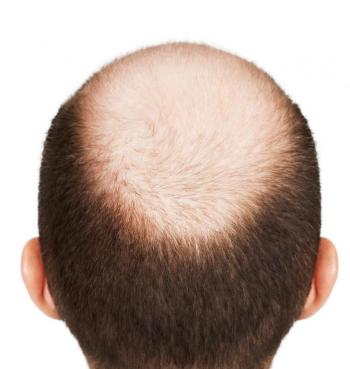
By looking to Figure 1, we can see that Male Pattern Baldness only affects hair on top of the head, while hair on sides and back does not fall. So, how can DHT cause hair in one area of the scalp to fall out but have no effect on hair follicles just a few millimeteres further down?
Figure 1 – Male Pattern Baldness, Norwood 7. Androgenetic alopecia affects only hair on top of the head. If DHT is the main cause of baldness, why hair on the sides and back are not susceptible to DHT? (From [60])Here is where the genetic part comes into action. According to the current theory, hair follicles on top of the head show increased expression of the androgen receptor gene [13], i.e. the top of the head is more sensitive to androgens action than hair on the sides and back of the head. However, higher levels of androgen receptors are also found in follicles of beard, scrotum and pubis, reinforcing the paradox [14]. Genetics also suggests that the probability of male pattern hair loss is dependent on family history and age [15]. However, in case of identical male twins, one can bald significantly faster than his counterpart [16]. These together with many other unknowns bring the necessity to define a new model for the explanation of baldness.
My studies on the subject started after a terrible personal experience (you can read my story here): a wrong splint therapy lead many symptoms to appear, among them tremendous muscular tensions in the neck. Muscles were so tight that I was exactly feeling their action propagating to the head and compressing the galea. This is when I started to lose hair at an incredible pace (Figure 2).
Figure 2 – On the left, healthy hair. On the right, my hair started to thin and to fall as a consequence of the muscle stiffness in the scalp.
I will then discover that muscles are connected together through myofascial connections and their action can be propagated in distal areas [17]. This is also what the trigger point model proposes: pain frequently radiates from points of local tenderness in muscles to broader areas, sometimes distant from the muscle itself [18]. By looking to Figure 3, we can clearly understand how action of neck muscles propagate to the head, so my feelings were actually right.
Figure 3 – Referred pains from upper trapezius, sternocleidomastoid, suboccipital, splenius capitis, splenius cervicis, semispinalis capitis,temporalis and masseter muscle trigger points. Crosses represents the location of the trigger point. Red area is the referred pain pattern for that specific trigger point. (From [18])Then another particular event happened. Neck muscles tensions kept increasing up to a point that they were so severe and unbearable that lying down on a bed was the only partial pain remedy. This is how I was forced to spend three months lying down on a bed, trying every possible remedy to relax the muscles. One of the most effective method was the transcutaneous electrical nerve stimulation (usually referred as TENS). I used it applied to neck muscles and it did relax them, although its benefits were very short in time. But I noticed an incredible fact: every time my 10-minute session ended, my hair was in a really good health. It was kind of surreal for me, how was this possible? Nevertheless, muscles were tightening again after a short time period and so my hair was affected too.
This gave me more inputs on where to look for to explain the mysteries behind hair loss: I understood that action of neck muscles propagates to the galea and that there was some connection. At that point, I did not know the actual mechanisms to explain how a compressed galea was causing hair loss but I understood it was the key. Galea’s key role can be simply guessed by looking to Figure 4: balding areas of Norwood 7 pattern exactly matches galea’s anatomy. Was this just a coincidence?
Figure 4 – On the left, Norwood 7 androgenetic alopecia. On the right, head and neck anatomy. Notice the bald area exactly matches the galea aponeurotica. (From [61])No, it was not a coincidence. As Figure 5 shows, blood vessels pass through all the scalp layers arriving to the hair follicles and one of these layers is the galea aponeurotica. If the galea is tightened, the blood vessels in the underlying tissues are compressed, i.e. blood cannot reach hair follicles causing reduced availability of oxygen, nutrients and inadequate removal of metabolites.
Figure 5 – Layers of the scalp. The epidermis, dermis, and galea glide over the pericranium as a fixed unit. Scalp vessels travel within the subcutaneous layer superficial to the galeal layer. (From [62])Not surprisingly, it has been found that subcutaneous blood flow in the scalp of patients with early male pattern baldness is much lower than the values found in the normal individuals [19]. This would explain the aforementioned higher formation of 5α-reduced metabolites and 17-ketosteroid metabolites at all sites of the scalp of bald men at the basis of the androgenetic theory.
The restriction in blood supply to tissues is called ischemia: this leads to insufficiency of oxygen (hypoxia). Not surprisingly again, men suffering from androgenic alopecia have significantly lower oxygen partial pressure (meaning microvascular insufficiency and hypoxia) in the areas of their scalp affected by balding (frontal and vertex regions) versus unaffected areas (temporal and occipital regions). Moreover, balding men have significantly lower oxygen partial pressure in the areas of balding scalp than the same areas of non-bald people [20].
Minoxidil solution, which is one of the commercially available medications for hair loss, stimulates the microcirculation of the bald scalp, effectively promoting hair growth [21]. Patients should be warned about increased shedding in the first months of treatment, that is seen as a positive response to the treatment [22]. How can this increased shedding be explained? Could it be the so called reperfusion injury, i.e. the tissue damage caused when blood supply returns to the tissue after a period of ischemia [23]?
In case of reduced blood supply, tissues are damaged and die, thus including the hair follicles and surrounding structures. A proof of this is the associated excessive dandruff found in hair loss [24]: the last layer of the skin, called stratum corneum, consists of dead cells (corneocytes) that are regularly replaced through desquamation. However, certain conditions trigger a more rapid turnover, leading to a larger shedding recognized as dandruff (Figure 6).
Figure 6 – Topical presentation of normal scalp and dandruff scalp. (From [25])When tissues are damaged, an inflammatory response is activated. The function of inflammation is to clear out necrotic cells and damaged tissues. The classical signs of inflammation are heat, pain and redness, situation recognized as scalp sensitivity (burning, stinging, dry scalp, vague discomfort in the scalp, and sometimes, trichodynia) that is associated with hair loss [26,27,28]. And guess what? Many studies have shown DHT plays an important role in inflammations, regulating its activity [29,30,31,32]. Could be this the explanation of why increased DHT levels are found in bald scalps?
When the inflammation is long-term and chronic, it causes fibrosis and calcification. Indeed, miniaturization of hair follicles has been associated with deposits of densely packed collagen bundles in the follicular dermal sheath, called perifollicular fibrosis [33,34,35]. This further decreases the blood flow into the scalp, promoting ulterior cells death.
So, I came to a conclusion: hair loss was not a problem of the hair itself but was a problem of the surrounding tissues. Take two seeds of a genetically identical corn, place one seed in a temperate climate and one in an arid climate: the one in the arid climate only grows to half the height of the one in the temperate climate due to lack of water and nutrients in its environment. This is exactly what happens with our hair and there are studies confirming it: miniaturized hair follicles of pattern alopecia can quickly regenerate once removed from the human scalp and can grow as well as or better than terminal follicles from the same individual [36]. And not only miniaturized hair can regrowth, but also terminal hairs can shrink in difficult recipient sites, impacting their growth and survival rates [37].
At this point, for me everything was clear. Only one thing was missing: where does this muscular tension come from? I will found out that craniofacial development has a huge impact on body posture and muscular balance. And actually all my symptoms were originating from a cranial distortion. Bingo! Now everything had an explanation!
Apparently, poor craniofacial development is a problem of civilized modern societies and not surprisingly also hair loss has widespread in the modern era. Figure 7 shows Native Sioux people that lived in the 19th Century. Their craniofacial development is something that would be considered extraordinary in our era, however at their time it was the normality. Also notice their perfect hair despite their old age. In Figure 8 we have instead a Sioux lived in our era, between the 20th and 21st Century: notice the difference in craniofacial development and the presence of hair loss.
Figure 7 – On the left, Red Cloud (1822-1909), leader of a Native American tribe (Sioux). In this picture he was 78 years old. Notice his excellent craniofacial development and how not surprisingly he has all his hair. On the right, another example of a good craniofacial development from the Sioux tribe lived in the same years. (From [63] and [64])Figure 8 – Russell Charles Means (1939-2012) was a Native American Oglala Sioux born in modern era. We can notice his poorer craniofacial development compared to his ancestors and his hair loss. (From [65])If we look to photographs taken over 100 years ago of Somalis in Figure 9, we can notice the excellent craniofacial development of the two individuals on the left and their perfect hair. However, the individual on the right has a poor craniofacial development and, not surprisingly, hair loss. In Figure 10, Barkhad Abdi, a Somali-American actor living in our era. Do you notice any difference with his ancestors?
Figure 9 – On the left, Warsame Yonis, 24 years old. In the middle, Igge Karbaashe, 20 years old and on the right Ali Gaboose, 20 years old. Notice the difference in Ali’s maxilla development and his hair loss. (From [66])Figure 10 – Barkhad Abdi is a Somali-American actor. Notice his much poorer craniofacial development compared with his ancestors and his hair loss. (From [67])Already in 1939 Weston A. Price wrote about his travel around the world where he discovered that jaw problems were not present in tribes of isolated areas far from civilization [38]. In a simplistic view, maxilla is primarily remodeled by forces coming from the tongue and teeth (through masseter muscles) and the causes of a poor craniofacial development have to be found in modern lifestyle, in particular in:
Increasing of bottle-feeding over breast-feeding that influences the swallowing pattern and all oral muscles [39,40,41,42].
Use of pacifiers/dummies that mainly affect tongue posture [43,44,45,46].
Trend towards industrial soft high-calorie food that hits chewing effort and muscles action [47,48,49].
Reduced nasal airways, increasing of allergies and nasal congestion that leads to mouth breathing affecting both tongue posture and muscles action [50,51,52,53,54].
Trend towards an earlier or too early weaning, influencing swallowing pattern [55,56].
When one or more of these factors are present, the maxilla drops down and back, reducing the eye support, flattening the cheekbones, narrowing the nasal airway, lengthening the mid facial third, and lowering the palate, which narrows and create malocclusion [57].
After discovering what a poor craniofacial development means for the hair, I started to look to every single person I was meeting, investigating their hair loss and the correlation with their jaws development: I never found a single bald person with a good craniofacial development! I also started to ask questions to people, curious to know the truth.
The first person I spoke with was my Portuguese housemate of that period. He had a very poor craniofacial development and he was bald. So I asked him: “Do you know if you used pacifiers or if you were bottle-fed when you were a child?”. His reply: “When I was a child, in Portugal it was almost a shame to breast-feed a child, so many mothers were opting to bottle-feed for this reason. My mother was one of those.”. No other comments are needed. Thus, I also started to ask the same questions to other people close to me: some have been breast-fed because their mother had not breast milk, some used pacifiers, some have been through a too early weaning and so on. There were no doubts that the correlation was clear.
I would like to show here some examples of famous people, so that everybody can understand what I am talking about. Figure 11 shows Prince William, Duke of Cambridge. On the left picture, you can clearly see his very narrow palate (i.e. a consequence of a poor craniofacial development). Also, if you pay attention, you will notice a cross-bite on one side and the dental midline that is shifted, sign of a cranial distortion. On the right picture, you can instead better appreciate his vertical growth of the maxilla, with missing cheekbones, missing support for the eyes, little lips, aquiline nose with little nostrils. I would not be surprised if he is a mouth-breather.
Figure 11 – Prince William, Duke of Cambridge. Notice in these two pictures his poor craniofacial development: vertical growth of maxilla, narrow palate, cross-bite on one side with dental midline shifted, little lips, aquiline nose with little nostrils. (From [68])In observing other people with hair loss problems, the more severe cases I have seen were for two reasons: either their craniofacial development was extremely poor or they had an impressive cranial distortion. Now, I want to show you what I mean. In Figure 12 we can observe Angelino Alfano (an Italian politician) and his really poor craniofacial development. On the left picture we can notice his really narrow palate and the midline that is not completely centered. On the right one, we can observe his excessive vertical growth of the maxilla, with consequences on his eyes, lips and nose shape.
Figure 12 – Angelo Alfano (Italian politician). Notice in these two pictures his extremely poor craniofacial development, notable from his excessive vertical growth of the maxilla, missing cheeckbones, eyes, nose and lips shape.
An example of an impressive cranial distortion is Jeff Bezos, current CEO of Amazon (Figure 13). In the left picture we can notice his narrow palate and also another important detail: look at his tongue, he has teeth signs on it. This means he has a tongue between the teeth posture, i.e. low tongue posture. In the right picture it is possible to notice his cranial distortion: asymmetrical face, asymmetrical ears, asymmetrical eyes, asymmetrical nasal philtrum and his mandible that deviates on one side.
Figure 13 – Jeff Bezos, CEO of Amazon. In the left picture notice his narrow palate and the teeth signs on the tongue, meaning a tongue between the teeth posture. On the right, notice his cranial distortion. with asymmetrical face, asymmetrical ears, asymmetrical eyes and his mandible that deviates on one side. (From [69])If craniofacial development is the key for hair loss, can we predict who will have predisposition for baldness once older? My answer is yes, however predisposition does not mean that hair loss will actually happen. Let us take an example, Dwayne Douglas Johnson, an American actor also known as The Rock (Figure 14). We can see him in his younger days on the left and notice his poor craniofacial development, highlighted by a vertical facial growth, missing eyes support, missing cheekbones. These clues are signs of his predisposition to baldness. Indeed, we better know him now with his bald head, as in the photo on the right, where we can also appreciate his asymmetric smile with a shifted midline.
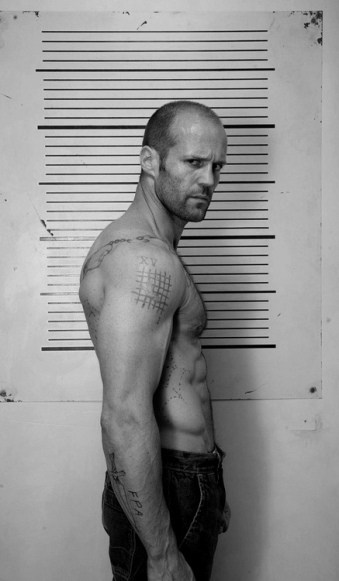
Figure 14 – Dwayne Douglas Johnson, aka The Rock. On the left, we can notice his poor craniofacial development, highlighted by a vertical facial growth, missing eyes support, missing cheekbones when he was young and still with hair. On the right, we can appreciate a more recent photo and his teeth asymmetry with a shifted midline. (From [70])The Rock played some movies with Jason Statham and I think he is also a good example for this theory. Notice in Figure 15 his posture with an increased kyphotic curve. Also notice the tightened muscles on the side of the neck while he turns his head, i.e. reduced neck mobility. If you investigate yourself, you will also find his excessive vertical growth of the maxilla, with a narrow palate, cross-bite on both side of the teeth and a cranial distortion.
Figure 15 – Jason Statham, English actor. Notice his posture with an increased kyphotic curve and the tightened muscles on the side of the neck while he turns his head, i.e. reduced neck mobility. (From [71])Another example: one day I was reading a newspaper and there was an article on the death of Danny Kirwan, guitarist of a British band named Fleetwood Mac. I did not know the band and neither him, but there was his picture when he was young that captured my attention (Figure 16).
Figure 16 – A young Danny Kirwan (1950-2018), known as guitarist of the Fleetwood Mac. In this picture we can notice his long hair but his poor craniofacial development. Once older, which implications this brings to his hair? (From [72])He had perfect long hair, but a pretty poor craniofacial development. So, will he be affected by hair loss once older? According to everything I knew, yes he will! So, curious to know the answer I searched a picture of him older and guess what? He suffered of baldness (Figure 17).
Figure 17 – An older Danny Kirwan (1950-2018), known as guitarist of the Fleetwood Mac. We can notice his baldness, that can be related to his poor craniofacial development. (From [73])Are you still with doubts? Then, I would like to put here a challenge. In Figure 18 there is Gianluigi Donnarumma, an Italian goalkeeper currently playing for AC Milan (2018), where we can notice his poor craniofacial development. He was born in 1999, so he is now 19 years old. Will he suffer of hair loss? Let us go back to this page in 10 or 15 years time, when he will be in his 30s, and we will probably have something new to discuss on.
Figure 18 – Gianluigi Donnarumma, Italian goalkeeper playing for AC Milan. He has a poor craniofacial development. In 10 or 15 years time, will he still have his hair? (From [74])
Summary: what this new model can explain
Now, let us put everything together and let us see how this new model can better explain predisposition to baldness, comparing it with the deficits of the androgenetic model, where DHT is thought to play a main role in the disease.
Hair follicles on top of the scalp are affected by androgenetic alopecia, while those on the sides are not.
Androgenetic model: hair follicles on top of the head show increased expression of the androgen receptor gene. However, DHT stimulates the production of pigmented terminal hair in many other areas after puberty and higher levels of androgen receptors are also found in these follicles which remain healthy, e.g. like in those in men’s beard. So, this is a paradox and thus the androgenetic model does not offer a clear explanation.
New model: neck muscular tension propagates through the myofascia to the galea, which tightens and compresses blood vessels going to the hair follicles. Instead on the sides of the head, the underlying tissue is made of muscles so it is softer and richer of blood vessels. Thus, a compression in those areas does not block blood reaching the follicles.
The incidence of Male Pattern Baldness increases with age. However, serum testosterone production declines with aging, together with lower serum DHT.
Androgenetic model: no explanation.
New model: neck muscular tensions that compress the galea are caused by an abnormal posture. Posture is determined by craniofacial development which depends on bone remodeling. Bone remodeling is a lifelong process, so an increase in age means a poor craniofacial development can worsen over time, with an impact on the posture. This creates higher predisposition to baldness with age.
Baldness have significantly spread in the modern era and isolated tribes are less likely to suffer of hair loss.
Androgenetic model: no explanation.
New model: craniofacial development depends on forces coming from orofacial muscles (among them, the tongue). The causes of a poor craniofacial development have to be found in modern civilized lifestyle (e.g. use of pacifiers, bottle-feeding, soft high-calorie diet, early weaning).
Subcutaneous blood flow in the scalp of patients with early male pattern baldness is much lower.
Androgenetic model: no explanation.
New model: galea compresses blood vessels, blocking blood flow.
Minoxidil solution stimulates the microcirculation of the bald scalp, effectively promoting hair growth.
Androgenetic model: no explanation.
New model: minoxidil acts as a vasodilator through membrane hyperpolarization caused by opening potassium channels [58,59]. This promote blood flow, thus hair growth.
The scalp of bald men show higher formation of 5α-reduced metabolites and 17-ketosteroid metabolites.
Androgenetic model: although DHT is considered playing the main role in baldness, this model does not give any explanation of why DHT and other metabolities should be present in higher concentration in bald scalps. So, no explanation.
New model: when blood vessels are compressed, blood cannot reach hair follicles causing reduced availability of nutrients and inadequate removal of metabolites, damaging tissues. Then, an inflammatory response is activated and DHT is an important regulator of its activity.
Excessive dandruff and scalp sensitivity are often associated with hair loss.
Androgenetic model: no explanation.
New model: dandruff consists of dead cells (corneocytes) from the last scalp layer that are regularly replaced through desquamation. In case of reduced blood supply, cells die more rapidly triggering an excessive turnover, i.e. the dandruff. When tissues are damaged, an inflammatory response is activated. The classical signs of inflammation are heat, pain and redness, situation recognized as scalp sensitivity (burning, stinging, dry scalp, vague discomfort in the scalp, and sometimes, trichodynia).
Miniaturization of hair follicles has been associated with deposits of densely packed collagen bundles in the follicular dermal sheath, called perifollicular fibrosis.
Androgenetic model: no explanation.
New model: when the inflammation is long-term and chronic, it causes fibrosis and calcification.
Conclusion
The model proposed on this website can explain many more things on baldness than the current androgenetic model can do. I am not here to say that it can fulfill all the unknowns of this disorder, but if the androgenetic model is accepted despite all its gaps then I do not see why this new model would not be considered and investigated. Anyway, the answer is in front of your eyes: just observe the craniofacial development and neck mobility of bald people and you will understand what I am talking about. You can contribute saying your opinion at the bottom of this page. I will try to clarify other aspects of hair loss in the second part of the article.
I found interesting your article at some points.
I have Androgenetic Alopecia.
Took finasteride, which works against 5a-reductase/ DHT reduction both scalp and serum, experienced regrowth and maintenance.
Had to stop the medication due to sides, lost all the progress and androgenetic alopecia kept pushing forward.
I think it is impossible to make those statement by looking at different people’s pictures. To be reliable you must took into consideration a greater, greater sample and judging non-discretionary. I can think about many men with a great cranial development and body development, but yet balding.
About your case, it could be a physiological receding hairline, effluvium etc.
Apparently some people are more sensitive to dht to others. In fact if there’s a history of balding in your family, chances of being sensitive to that is most likely to happen.
It is known that Minoxidil alone, doesn’t do anything in the long term, and even finasteride on the long term becomes ineffective.
Quite few people already, some time ago researched about cranial exercises with the only hair growth purpose, without unfortunately any success.
There are many logical facts that actually make this castle fall.
Just a simple one.
Men who undergo hair transplant procedure, with their hair follicles transplanted from below the galea aponeurotica to the top of galea aponeurotica, following one of the stated reasoning everyone of them should go bald again in the receiving area. But it doesn’t happen.
Unfortunately that does not seem to be true. Research studies I have found assess hair transplants after 1 or 2 years, while it would be important to do it after 5, 10 or 15 years. If what you say was true, then we would not see all these people complaining in forums about hair transplants and their ineffectiveness after many years (I am active followers of forums and blogs on hair loss).
I believe that the craniofacial development has a lot to do with baldness, but if this model is indeed the true cause. How do you fix it for the men alive today? I believe there is a way, but I would like to hear what your ideas are on that. Again, ideas on how to help MEN TODAY, not change how children are swallowing and posturing their tongues.
Damn the entire allopathic medical field of study, it has done much more harm than good. Nature has the answers, but we try to steal from nature in order to profit. Pacifiers and bottle feedings, ideas stolen from nature, and look at the people of the world suffering because of it.
Unfortunately I don’t think the general public is fit to find a solution. But just finding these possible connections between posture and hair loss should hopefully be enough to spark some interest in the science communities.
I really wanted to believe that but unfortunately it is not possible. Take Mike Mew for example, who is the biggest promoter of these things about craniofacial development. He was treated at the age of 5 by his father, he certainly has beautiful facial development and posture but he is BALD while his 93 year old father has a full head of hair. Also, how is it possible to explain my case? My hair started shedding like hell just a few months after I turned 17. No event that could significantly alter the muscle pressure in my neck, as far as I can remember. It’s your genes, man. It is painful to accept but that is it.


















Very very interesting!
LikeLike
What would be a possible form of treatment?
LikeLike
I found interesting your article at some points.
I have Androgenetic Alopecia.
Took finasteride, which works against 5a-reductase/ DHT reduction both scalp and serum, experienced regrowth and maintenance.
Had to stop the medication due to sides, lost all the progress and androgenetic alopecia kept pushing forward.
I think it is impossible to make those statement by looking at different people’s pictures. To be reliable you must took into consideration a greater, greater sample and judging non-discretionary. I can think about many men with a great cranial development and body development, but yet balding.
About your case, it could be a physiological receding hairline, effluvium etc.
Apparently some people are more sensitive to dht to others. In fact if there’s a history of balding in your family, chances of being sensitive to that is most likely to happen.
It is known that Minoxidil alone, doesn’t do anything in the long term, and even finasteride on the long term becomes ineffective.
Quite few people already, some time ago researched about cranial exercises with the only hair growth purpose, without unfortunately any success.
LikeLike
There are many logical facts that actually make this castle fall.
Just a simple one.
Men who undergo hair transplant procedure, with their hair follicles transplanted from below the galea aponeurotica to the top of galea aponeurotica, following one of the stated reasoning everyone of them should go bald again in the receiving area. But it doesn’t happen.
LikeLike
Unfortunately that does not seem to be true. Research studies I have found assess hair transplants after 1 or 2 years, while it would be important to do it after 5, 10 or 15 years. If what you say was true, then we would not see all these people complaining in forums about hair transplants and their ineffectiveness after many years (I am active followers of forums and blogs on hair loss).
LikeLike
Why do you think that male pattern baldness is associated with high blood pressure, coronary heart disease and an increased risk of prostate cancer.
LikeLike
I believe that the craniofacial development has a lot to do with baldness, but if this model is indeed the true cause. How do you fix it for the men alive today? I believe there is a way, but I would like to hear what your ideas are on that. Again, ideas on how to help MEN TODAY, not change how children are swallowing and posturing their tongues.
Damn the entire allopathic medical field of study, it has done much more harm than good. Nature has the answers, but we try to steal from nature in order to profit. Pacifiers and bottle feedings, ideas stolen from nature, and look at the people of the world suffering because of it.
LikeLike
Unfortunately I don’t think the general public is fit to find a solution. But just finding these possible connections between posture and hair loss should hopefully be enough to spark some interest in the science communities.
LikeLike
I really wanted to believe that but unfortunately it is not possible. Take Mike Mew for example, who is the biggest promoter of these things about craniofacial development. He was treated at the age of 5 by his father, he certainly has beautiful facial development and posture but he is BALD while his 93 year old father has a full head of hair. Also, how is it possible to explain my case? My hair started shedding like hell just a few months after I turned 17. No event that could significantly alter the muscle pressure in my neck, as far as I can remember. It’s your genes, man. It is painful to accept but that is it.
LikeLike
explain then why it hair loss only affects hair on the scalp
LikeLike
What would be a possible form of treatment?
LikeLike