Our body perfectly functions only if fully aligned. There is no other way! The quality of our life strictly depends on the spinal alignment, so our posture is a key element for being in a good state of health.
Every single moment, our body fights an invisible force to stay upright: the gravity. The brain continuously works to find our body’s position in the space, i.e. the posture. Roger Sperry (Nobel Prize in Physiology and Medicine in 1981) discovered that 90% of the
brain’s activity is used to balance our body within the gravitational field of earth. If our body is mechanically distorted, it will affect the other 10% of the brain’s activity, which controls all the other body functions such as breathing, digestion and cognition [1].
The pillar of our posture is the spine (Figure 1), that is held in place by the soft tissues of the body, i.e. muscles, tendons, ligaments and fascia. Take all the soft tissues away and the bones would pile on the floor, as they do not interlock or stack in any kind of stable way.
Figure 1 – Anatomy of the spine. The spine is the central support of our bodies. Made up of bones called vertebrae, and separated by cushions called discs, our spines also house the bundle of nerves responsible for our movements, called the spinal cord. (From [57])The position of the bones depends on the tensional balance among soft tissue elements. In order to guarantee body balance, the myofascia (a thin layer covering and connecting muscles) in a human body has intrinsic tone and is never completely lax (stress/strain can never reach zero): the integrity lies in the balance of tension, named tensegrity. Forces are distributed throughout the system rather than locally concentrated and the musculoskeletal system therefore functions as a single unit [2]. As gravitational forces act upon our bodies when we are upright, various groups of musculature work synergistically so that we can stay erect (Figure 2).
Figure 2 – Major antigravity muscles that synergistically work for our erect posture. The position of the spine depends on the tensional balance among these groups of muscles. (From [58])As gravity acts on all parts of the body, one’s entire weight can be considered as concentrated at a point where the gravitational pull on one side of the body is equal to the pull on the other side. This point is the body’s center of gravity, and it constitutes the exact center of body mass (Figure 3). When the center of gravity is above the base of support and the pull of gravity is successfully resisted by the supporting members, an equilibrium of forces or a state of balance is reached and no motion occurs [3]. The line of gravity is considered to run anterior to L4-5, but it moves naturally with changes in spinal alignment. In particular, as inclination of the trunk increases, the gravity line moves further anterior, with muscles of the back that must counteract the change in the center of gravity [4], with following back pain [5].
Figure 3 – Line of gravity in a body structure. The center of gravity runs anterior to L4-5. (From [59])But where do our postural problems originate? Our body is a complex but perfect system, with many inputs and outputs. The posture is an output of this system, with inputs coming from vestibular, visual and somatosensory systems [6,7], with this last one including proprioception (Figure 4). Proprioception is the awareness of the position of one’s body, possible with stimulus coming from nerves throughout our entire body. Occlusion is part of the proprioceptive inputs.
Figure 4 – Body balance is controlled by three sensory systems: vestibular, visual, proprioceptive. (From [60])Under the hypothesis of sensory reweighting, every input has a weight when processed by our brain. When a certain input is distorted or missing, the system rebalances the weight of other inputs or even suppresses some of them when they are in conflict, so that the body is always in the most stable position [8,9,10]. This has been proved by many studies, with body posture that changes according to different vision stimulus [11] or different occlusion contacts [12,13,14]. However, occlusion is just the consequence and adaptation of the cranial situation [15]. See in Figure 5 the direct relationship between cranial distortions and occlusion.
Figure 5 – On the left, relation of cranial base with maxilla and mandible in case of left sidebending. Occipital bone and mandible are sketched with the same red colour since they relate each other, while maxilla and sphenoid are in blue. On the right, the relative dentition that correspond to the cranial pattern shown on the left. (From [15])The maxilla remodels according to forces coming from the tongue and the teeth in contact. When these forces are missing, the maxilla remodels down and backward, elongating the facial shape. As a consequence, the mandible swings back and the body reacts with a forward head posture [16], as can be seen in Figure 6.
Figure 6 – Two patients from study [16]: subject HB003 shows vertical growth of maxilla, with facial retrognathism and large mandibular inclination. Notice the forward head posture and the reduced airways’ space. Subject HB092 shows forward growth of maxilla, with facial prognathism and small mandibular inclination. Notice the head posture aligned with the cervical column and the bigger space for the airways.With a forward head posture, increasing the kyphotic and then lordotic curves is the only way the body has to find the center of gravity [17,18]. With an increased lordosis, also the pelvis rotates forward, with consequences until the feet [19]. Figure 7 shows different body postures according to different classes of malocclusion: notice the different head posture and following compensatory mechanisms to find the center of gravity.
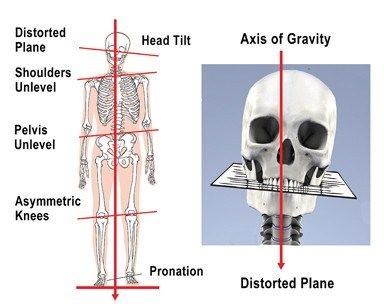
Figure 7 – Different malocclusion classes relate to different body postures. (From [61])In the presence of cranial distortions, the mandible deviates to one side as a consequence of the occipital bone position, while the maxilla rotates to the other side, mapping the sphenoid bone. As a consequence, facial features are asymmetrical and the head is tilted on one side [15]. The shoulder where the head is tilted lifts up to level the eyes. Then, the body has to compensate, creating a scoliotic curve [20,21]. As a consequence, the hips are not aligned, giving the impression of a leg shorter than the other. However, the real length of the legs is the same, they are just asymmetrically aligned, as Figure 8 highlights.
Figure 8 – In case of cranial distortions, the head tilts on one side. The shoulder where the head is tilted lifts up to level the eyes, with following scoliotic curve and hips that are not aligned. (From [62])If kyphosis, lordosis and pelvis anteversion are adaptation of the body in the sagittal plane, tilted head, unlevel shoulders, scoliosis, unlevel hips are adapatation on the frontal plane. However, we still miss one plane: the transversal or horizontal plane (Figure 9).
Figure 9 – There are three anatomy planes of the body: sagittal, horizontal and frontal. (From [63])In the presence of cranial distortion, the skull is twisted, with sphenoid and occipital bones in opposite rotation. Then, this is also reflected in all the spine: indeed, in the presence of scoliosis there is also vertebrae rotation on the transversal plane [22,23], together with rotation of the pelvis (Figure 10) [24].
Figure 10 – Scoliosis has to be considered on both frontal and transversal planes. Although scoliosis is mainly associated to a lateral sway of the spine and uneven pelvis, scoliosis also involves a vertebral and pelvic rotation on the horizontal plane. (From [64])Our body better functions when it is aligned, on all the three planes. If not aligned, the body suffers, full stop! For every centimeter that the head is held forward (rather than balanced properly over the body), it gains about 2 kg of weight, with muscles of the back and neck that have to work much harder [25]. Here is the link between forward head posture and reduced neck mobility [26], neck pain [27,28], migraine [29] and tension-type headache [30] and the link between scoliosis and pain in several anatomical locations [30,31,32].
But in all of this, we still miss the bigger pictures. What happens when there is chronic tension in certain muscles? What happens when spine is not aligned and vertebrae are dislocated or subluxated? In our body we have blood vessels, nerves, glands, organs that can be compressed by either muscles that are overtightened or by vertebrae misalignment (Figure 11).
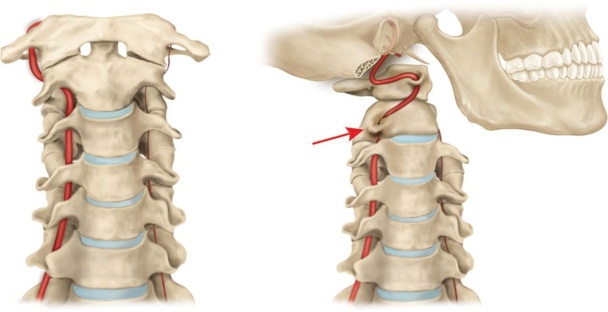
Figure 11 – Our spine is surrounded by many blood vessels and nerves. The spinal cord is a long, thin, tubular bundle of nervous tissue from which all the nerves propagate. It passes through the vertebral canals from the occipital bone to the lumbar vertebrae. (From [65,66])Think for example about large blood vessels going to the brain that can be compressed by neck muscle tension (Figure 12) [34,35], arteries that can be compressed by vertebral rotation (Figure 13) [36,37,38], the spinal cord that can be compressed by vertebral dislocation or subluxation (Figure 14) [39], lungs that have decreased capacity with an increased kyphosis [40,41], or about duodenum compression as a consequences of increasing lordosis or scoliosis [42].
Figure 12 – The jugular veins are veins that take deoxygenated blood from the head back to the heart via the superior vena cava. The external jugular vein runs superficially to sternocleidomastoid, while the internal jugular vein runs in the carotid sheath, that is a connective tissue part of the deep cervical fascia. (From [67])Figure 13 – Example of rotational vertebral artery occlusion. On the left, stenosis (narrowing) or anomaly of the vertebral artery on one side. On the right, compression of the dominant vertebral artery at the C1-2 level during contraversive head rotation. (From [43])Figure 14 – Example of spinal misalignment with vertebral dislocation compressing the spinal cord. (From [68])Consequences are disrupting. The restriction in blood supply to tissues is called ischemia: this leads to insufficiency of oxygen (hypoxia), reduced availability of nutrients and inadequate removal of metabolites. This damages the tissues and an inflammatory response is activated. Inflammation is a defense mechanism in the body in which the immune system clears out necrotic cells and damaged tissues. However, if the blood vessels compression is chronic, then inflammation becomes chronic too, with following fibrosis and calcification.
Current medicine considers an autoimmune disease, e.g. Multiple Sclerosis, as a condition in which the immune system mistakenly attacks the body, causing an inflammation [44,45]. However, are we sure that the inflammation is the consequence and not the cause of the disease? After all, Multiple Sclerosis has been linked to CCSVI (chronic cerebrospinal venous insufficiency) [46,47], that is a reduced blood flow from the brain and spinal cord due to narrowing of veins in the neck.
Furthermore, many other diseases have blood flow that plays a major role. To cite some:
The subcutaneous blood flow in the scalp of patients with early male pattern baldness is much lower than the values found in the normal individuals [48], with lower oxygen partial pressure (meaning microvascular insufficiency and hypoxia) [49].
Severity of schizofrenia can be predicted by meaning of blood flow within the brain [50].
People with stuttering have a lower regional cerebral blood flow in Broca’s area [51].
Patients with mild cognitive impairment, dementia and Alzheimer’s disease have a reduced cerebral blood flow [52,53], with the entire brain that is degraded, resulting in tissue loss (Figure 15).
Figure 15 – Brain atrophy in advanced Alzheimer’s Disease. In an Alzheimer’s patient, the entire brain is degraded resulting in tissue loss. The cortex of the brain shrivels up, which damages the ability of the brain to think, plan, and remember. (From [69])Current medicine still focuses too much on isolated parts of the body, lacking the consequences that these parts can have in distal locations. Posture has an important role in body’s health that can be truly understood only in a holistic approach. Spinal posture is what determines the dependence in activities of daily living [54] and our life satisfaction [55] when we become older. Spinal posture is also what predicts our mortality [56] and after having read this page we should all know why: alignment is the key for body’s health, do not forget it!
Poor body posture is a very frequent problem in modern days: forward head posture, rounded shoulders, the appearance of a little hump and of a belly fat, even if you are really young and skinny. From sedentary life to excessive use of mobile phone, from being seated most of the day to psychological reflexes, many…
4 thoughts on “Body Posture: Alignment Is The Key for Health”
hi,
thank you for your extreme informative and well-researched website. also your personal story really touched me and I feel you are really strong to have lived through so much pain!
I really want to recommend you the Gokhale method for relearning natural posture. the book is amazing and there are a few youtube videos. also sleeping like this WITHOUT a pillow really helped me. https://de.gokhalemethod.com/blog/67445
and rubbing like a bear with a foam roller on the wall! 🙂
do you do anything else but mewing? do you get more treatment for your teeth?
Hi TMD, great article you made about body posture and the Importance of it.
But I do have a question after reading this article.
If I am trying to fix my body posture then should I work my muscles and the myofascial meridian lines of my back,head, and everywhere else. Or fix my tongue posture to bring the maxilla up and forwards first to give me good body posture?
I understand this is explaining the cause of how posture affects and unraveling the truth of what really causes bad body posture and not giving a solution. But I do like you share and I hope your info goes widespread and change the whole medical industry
Your website is really amazing, I hope you find more time to complete the other sections. It greatly helps me to understand my young yet screwed up body…
Your analysis on this topic is mind blowing and you have cleared each and every point with well defined way !!
Ping me if you share any other info like this

















hi,
thank you for your extreme informative and well-researched website. also your personal story really touched me and I feel you are really strong to have lived through so much pain!
I really want to recommend you the Gokhale method for relearning natural posture. the book is amazing and there are a few youtube videos. also sleeping like this WITHOUT a pillow really helped me. https://de.gokhalemethod.com/blog/67445
and rubbing like a bear with a foam roller on the wall! 🙂
do you do anything else but mewing? do you get more treatment for your teeth?
warm regards!
LikeLike
Hi TMD, great article you made about body posture and the Importance of it.
But I do have a question after reading this article.
If I am trying to fix my body posture then should I work my muscles and the myofascial meridian lines of my back,head, and everywhere else. Or fix my tongue posture to bring the maxilla up and forwards first to give me good body posture?
I understand this is explaining the cause of how posture affects and unraveling the truth of what really causes bad body posture and not giving a solution. But I do like you share and I hope your info goes widespread and change the whole medical industry
LikeLike
Your website is really amazing, I hope you find more time to complete the other sections. It greatly helps me to understand my young yet screwed up body…
LikeLike
Your analysis on this topic is mind blowing and you have cleared each and every point with well defined way !!
Ping me if you share any other info like this
LikeLike