Craniofacial Development: Malocclusion Is Just A Symptom
When talking about malocclusion, crooked teeth are the first thing that comes in mind. However, malocclusion is just a sign of something bigger: an incorrect development of the entire craniofacial complex, that in turn affects total body health. Bones remodel according to force stimulus: when it comes to maxilla, the main factors are the forces coming from tongue and teeth (through masseter muscles). So, when the natural tongue posture and swallowing pattern are affected, together with the muscle tone of the entire orofacial complex, the maxilla drops downwards and backwards. As Figure 1 highlights, this reduces the eye support, flattens the cheekbones, narrows the nasal airway, lengthens the mid facial third and lowers the palate, which narrows and create malocclusion.
Figure 1 – Tongue posture directly affects maxilla remodeling. When the tongue is correctly on the roof of the mouth, maxilla is remodeled up and forward (above case). Instead, when the tongue is not in the correct position, maxilla misses its forces and remodels down and back (bottom case). Notice the difference in cheekbones, eyes support, nose shape, length of the face and lips shape. (Adapted from [1] and [7]).These concepts are still unknown to many doctors or they are hidden for conflicts of interests. Indeed Figure 2 shows a patient before a surgery to correct his facial discrepancy. However, notice his tongue posture: tongue should rest on the roof of the mouth, remodeling the maxilla up and forward with its forces. But, for this individual, the tongue is low, with maxilla missing the support and forces from the tongue, that instead remodels down and backwards. Here is the origin of his Class III malocclusion. Notice the flat and long face, the absence of cheekbones, the wide eyes and narrow nostrils.
Figure 2 – Patient with Class III malocclusion before receiving surgery for his facial discrepancy. However notice his low tongue posture, the real cause of his facial shape and malocclusion. (From [2])Unfortunately, the current conception in medicine sees every part of the body individually, sometimes treating just the symptoms, but not the real causes. On the contrary, the body is an unique system and has to be approached in a holistic manner. There are blood vessels, nerves, muscle chains, tissues, bones, etc that run throughout the entire body, interacting and influencing each other. So, when talking about malocclusion, every single aspect has to be taken into account, starting from the tongue action arriving to maxilla development that has to be considered in the entire body context.
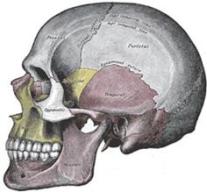
As said, occlusion is just a consequence of the entire craniofacial development: indeed maxilla is directly connected to the sphenoid and vomer bones, that in turn are connected to frontal, parietal, ethmoid, temporal, zygomatic, palatine and occipital bones, as Figure 3 highlights. These bones are joined together thanks to sutures: these sutural areas contain blood vessels, nerve plexuses, connective tissue, Sharpey’s fibers and red blood cells [3].
Figure 3 – Medial view of sagittal plane of the skull. Notice how all the bones are directly or indirectly connected together. (From [8])In the total scheme of body design, cranial sutures role is to join other cranial bones together but primarily serve as expansion-contraction joints to allow accommodation for changes in meningeal, muscle and fascial tensions, respiratory and cardiac rhythms and alterations in both cerebrospinal and blood pressure [4]. Furthermore sutures also function as intramembranous bone growth site that respond to force stimuli, contributing to the morphogenesis of the bones of the cranial vault and facial complex [5].
According to this, it should be easy to understand that if maxilla develops incorrectly, then all the others cranial bones are affected as well. Their position changes according to the acting forces and thanks to the mobility offered by sutures, in order to establish an equilibrium state. Figure 4 shows the relationship between the basicranium (occipital and sphenoid bones) with the jaws (maxilla and mandible) and how they directly influence each other. Then all the other cranial bones are affected as well and, furthermore, the basicranium is also in relationship with the spine, influencing total body posture.
Figure 4 – Relationship of the basicranium (occipital and sphenoid bones) and the jaws (maxilla and mandible). (From [9])For a good clinician who understands all these concepts, it is easy to determine the cranial situations and the presence of cranial strains and/or distortions just looking to the occlusion and the palate. In the following, a good example of cranial distortion is taken from the article Correction of Dental and Cranial Sidebend with ALF by dentist Dennis Strokon [6]. The case shown in Figure 5 has a sidebend distortion, in which there are two factors involved: rotation of the cranial base occurs in both horizontal and vertical planes. Looking to facial features, the left side of the face is visibly narrower than the right. The left eye is lower than the right. The left ear is lower and more flared than the right ear. The upper facial midline deviates to the right and the philtrum of the upper lip is also off to the right. This facial features corresponds to an occlusion that is asymmetric Class II, with Class II molar and cuspid relationship on the left and Class I molar and cuspid on the right, leading to a mandibular centerline that is displaced toward the left.
Figure 5 – Patient with left sidebend. Notice his asymmetrical facial features that correspond to the shown occlusion. (From [6])The sidebending presents a certain occlusion that directly relates to the position of the cranial base. Figure 6 shows the sphenoid and occipital bones, in relation with maxilla and mandible. Maxilla and sphenoid bone are shown in the same blue colour since they directly influences each other, while occipital bone and mandible are in red. The corresponding dentition is the one present on the right of Figure 6.
Figure 6 – On the left, relation of cranial base with maxilla and mandible in case of left sidebending. Occipital bone and mandible are sketched with the same red colour since they relate each other, while maxilla and sphenoid are in blue. On the right, the relative dentition that correspond to the cranial pattern shown on the left. (From [6])The article better explains every single detail of this case of left sidebending. It has been cited here to highlight that occlusion and the overall craniofacial development cannot be seen individually. In addition, since the body is a unique system, this is then reflected in the total body health (including physical, emotional, spiritual and mental parts).
A doctor/dentist/orthodontist that does not know these concepts cannot be considered fully reliable. Occlusion is the results of forces balance. Its modification means to change this equilibrium and, if done wrongly, the consequences are devastating and reflected in the total body. Furthermore, prevention is much more important than correction in older individuals. Knowing the causes of malocclusion, particular attention has to be paid from the very first moment of life of a new born, avoiding actions that then becomes habits maintained for the entire life of the individual, affecting his entire health.
Just want to say thank you for posting all of this. This has aligned with everything I learned about mewing, orthotropics, and my own craniofacial journey. Please keep up the good work!
Premolar extraction followed by retraction of the jaw is a barbaric, torturous treatment to fix a simple overbite. It is done on people all over the world by stupid orthodontists that now nothing but moving teeth. It’s psychotic, idiotic and it ruins peoples lives, worst outcome is death/suicide. This is the results of the orthodontists greediness for money.







Do you recommend Invisalign to fix uneven teeth lining?
LikeLike
Just want to say thank you for posting all of this. This has aligned with everything I learned about mewing, orthotropics, and my own craniofacial journey. Please keep up the good work!
LikeLike
Premolar extraction followed by retraction of the jaw is a barbaric, torturous treatment to fix a simple overbite. It is done on people all over the world by stupid orthodontists that now nothing but moving teeth. It’s psychotic, idiotic and it ruins peoples lives, worst outcome is death/suicide. This is the results of the orthodontists greediness for money.
LikeLike
Thank you for sharing thhis
LikeLike