Genetics is everywhere. Genes contain all the information an organism uses to function (genotype) and they are handed down from parents to offspring. However, organism’s observable characteristics or traits (phenotype) depends from the combination of genetic processes with an organism’s environment and experiences that influence its development and behavior. Take two seeds of a genetically identical corn, place one seed in a temperate climate and one in an arid climate. Do you think they will grow in the same way? Although genetics would set the two plants to grow almost identically, the one in the arid climate only grows to half the height of the one in the temperate climate due to lack of water and nutrients in its environment. While current medicine mainly talks about genetic factors in many diseases, we should remember that man also is affected by environmental factors. So, what is the limit between the effect of genetics (nature) and environment (nurture) on humans? Is genetics really to blame for all the modern diseases? Read through and you will discover part of the truth.
Although genes contain all the information an organism uses to function, the environment plays an important role in determining the ultimate phenotypes an organism displays. Tropism in plants indicates the movement in response to an environmental stimulus [1]. In phototropism, shoots grow in the direction of the light source, since it is its main source of energy. In gravitropism, roots grow in the direction of gravitational pull (i.e., downward) and stems grow in the opposite direction (i.e., upwards, Figure 1). Also, in autotropism, proprioception is the ability of plants to perceive their own deformations, stimulating straightening of a curved organ. In natural conditions, the three processes interact constantly.
Figure 1 – Example of gravitropism. (From [45])Man is not different. Our parents give us the genetic traits, the growing path. This path is then followed or not depending on the environment. Take twins: sun exposure and smoking have an impact on facial appearance (Figure 2), with just a 5-year difference in smoking history producing noticeable differences in their faces [2].
Figure 2 – At age 61, identical twins Jeanne (on the left) and Susan no longer look exactly alike. Susan (on the right) smoked for many years and is an admitted sun worshipper, habits Jeanne does not share.(From [46])Current medicine labels many diseases, disorders and syndromes with genetic etiology. However, many of them only spread in recent times. So, are we sure it is really genetic?
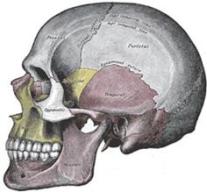
Malocclusion is one of these problems believed to be genetic. It is becoming so common in our modern society that almost everyone thinks having a brace is a step strictly required throughout our life. However, if we look to our ancestors (the origin of our genes), there is very little sign of malocclusion [3]. Figure 3 shows the difference of a prehistoric skull against a modern one: the difference in the palate shape and airways size is massive. So, is it really genetic?
Figure 3 – On the left, prehistoric skull: notice the large flat U-shaped palate and bigger airways. On the right, a modern skull with narrow high v-shaped palate and reduced airways. (From [3])Luckily many doctors (John Mew and Weston A. Price among these) questioned the etiology of malocclusion, concluding that it is a consequence of poor craniofacial development: bones remodel according to force stimuli that in case of maxilla are primarily coming from the tongue and the teeth (through masseter muscle). Bottle-feeding, pacifiers, industrial soft high-calorie food, mouth breathing, too-early weaning are common features of modern society determining the causes of jaw problems. Moreover, as usually happens with modern medicine, only symptoms are treated: when wearing braces, teeth are straightened but the underlying jaw problem is not resolved. This means either a retainer is needed for the rest of the life or the final result will relapse [4]. By instead treating the underlying problem, no relapse happens in the future, as in the case of patients treated by John Mew (Figure 4).
Figure 4 – Patient treated by John Mew with Orthotropics, by correcting the facial growth. Notice how correcting the jaw problem results in a correction of the malocclusion problem, with no future relapse.
Many other diseases are considered genetic, despite several clues supporting the opposite. Hair loss is one of these and it exponentially spreads in last decades. According to the current medicine, the typical male pattern baldness, characterized by hair on the sides and bald on top, depend on the miniaturization of genetically programmed hair follicles driven by activity of the dihydrotestosterone (DHT). Hair follicles on side would be genetically different and resistant to DHT action. But if this is true, why, once transplanted on the top, these terminal hair starts to fall again after some time, leaving patients as in Figure 5? And why vellus hair (miniaturized, balding) regenerates just as well as or even better than terminal hair (hairy, nonbalding) when transplanted in similar environments [5]?
Figure 5 – Head with hair loss and scar from hair transplant. (From [47])The simple answer is that genetic plays a little role in male pattern baldness. Indeed, a poor craniofacial development leads to poor body posture with abnormal tension of neck muscles. This tension propagates to the galea aponeurotica (Figure 6) that tightens and compress blood vessels, causing fibrosis and calcification that further tighten the galea. Hypoxia (oxygen deficiency in the tissues) causes the death of hair follicles, thus hair loss. It is a confirmation the fact that blood flow in scalp of balding people is significantly lower than the one in normal people [6]. Furthermore, men suffering from androgenic alopecia have significantly lower oxygen partial pressure (meaning microvascular insufficiency and hypoxia) in the areas of their scalp affected by balding (frontal and vertex regions) versus unaffected areas (temporal and occipital regions) [7]. Also, by relieving tension at the vertex in the scalp, cutaneous blood flow rate increases, promoting hair regrowth [8,9].
Figure 6 – The galea aponeurotica is attached to the occipitofrontalis muscles and to the temporalis muscle via the temporalis fascia. Neck muscle tension propagates to the head, causing the galea to tighten, promoting loss of hair in the typical male pattern baldness. (From [48])Poor body posture may be responsible for many other disorders. We have muscle chains that run throughout our body, tightening and compensating to maintain a stable posture, and bones that can twist or rotate, like in the case of vertebrae rotation. And there are blood vessels, nerves, glands, organs that can be compressed by either overtightened muscles or by bones and vertebrae misalignment.
Stuttering is largely thought to be genetic. However, a recent research found out that people with stuttering have a lower regional cerebral blood flow in Broca’s area [10]. Is this genetic? Remember that we have large blood vessels going to the brain that can be compressed by neck muscle tension [11,12] and arteries that can be compressed by vertebral rotation [13,14,15]. Could be this also the cause of also many other syndromes arisen in modern times? Multiple Sclerosis has been linked to CCSVI (chronic cerebrospinal venous insufficiency) [16,17], that is a reduced blood flow from the brain and spinal cord due to narrowing of veins in the neck, in particular of the jugular veins. Patients with mild cognitive impairment, dementia and Alzheimer’s disease also show a reduced cerebral blood flow [18,19], with the entire brain that is degraded, resulting in tissue loss (Figure 7).
Figure 7 – Brain atrophy in advanced Alzheimer’s Disease. In an Alzheimer’s patient, the entire brain is degraded resulting in tissue loss. The cortex of the brain shrivels up, which damages the ability of the brain to think, plan, and remember. (From [49])Carpal tunnel syndrome is the disability that results from the median nerve being pressed or squeezed, causing numbness, tingling, or burning sensations in the thumb and fingers, with pain in the wrists or hands, loss of grip strength and loss of manual dexterity. The major risk factor for carpal tunnel syndrome is considered genetic. However, poor body posture, especially in cases of forward head posture, implies protracted shoulders, increasing strain on the various nerves passing through the shoulder region. One of these nerves is indeed the median nerve. Did you know that carpal tunnel syndrome is associated with forward head posture [20]?
Figure 8 – There are two main nerves that service the arm, the median and the ulnar nerves. Both flow out from the neck and make their way down through the upper extremity. Carpal tunnel syndrome derives from median nerve compression in the shoulder area. (From [50])In many cases of TMJ internal derangement, the auriculotemporal nerve (a small branch of the mandibular nerve) can become drawn into the compression zone of the TMJ, with possible neuroinflammation. This neuroinflammation may spread and could act as physiological drivers for aberrant reflexive behaviors, arising movement disorders, e.g. dystonia, Tourette’s syndrome [21,22]. Being the TMJ in direct relationship with the cranial structure and body posture, many other disorders are linked to TMD, such as fibromyalgia [23] and multiple sclerosis [24].
Genetics is also considered to play an important role in obesity. As Figure 9 shows, obesity has been linked with an increased risk of developing insulin resistance and type 2 diabetes [25], increased risk of hypertension [26] and cardiovascular disease (e.g. heart failure, coronary heart disease, sudden cardiac death) [27], cancer [28], mental disorders [29] and higher mortality [30,31].
Figure 9 – Co-morbidities associated with overweight and obesity. (From [32])
If you believe that all of this is related to bad genes, then it is better that you reconsider your thoughts: remission of type 2 diabetes comes from changing dietary and physical activity habits [33]; healthy food can reduce hypertension by 21 mmHg (drugs usually reduce it by 10-15 mmHg) [34,35]; fruit and vegetables have a strong protective effect against cardiovascular diseases [36,37], cancer [38,39] cognitive decline [40,41] and all-cause mortality [42,43]; increased consumption of whole grains has been associated with reduced risk of major chronic diseases including cardiovascular disease, type II diabetes, and some cancers [44].
So, is genetic really to blame for many modern syndromes? This article has not been written with the purpose of voiding genetic factors in the etiology of many diseases. Genetics is present in everything. The purpose of this article is trying to educate people in the pursuit of the truth, giving emphasis to the environmental causes that have been widely suppressed, hidden or forgotten by the current medicine. Remember that there is always a reason for everything!