Breathing is one of the basic vital function of our body and, thanks to the nose, it should be as simple as that. In reality many people suffer of breathing problems, like mouth breathing, asthma, sinusitis, snoring and sleep apnoea. So, why breathing through the nose is so important but many people cannot do it properly?
Every cell in your body intakes the oxygen and releases the carbon dioxide, in a process called cellular respiration (Figure 1). Breathing is important because our cells constantly need a new supply of oxygen so they can produce energy. Without this vital oxygen, cellular function is impaired, and damage or cell death is possible.
Figure 1 – Cellular respiration is the process of breaking sugar (glucose) into a form that the cell can use as energy (ATP, adenosine triphosphate). This process uses oxygen and is called aerobic respiration. It also produces carbon dioxide as a waste product, which is then taken to the lungs, where it is exchanged for oxygen. (From [39])The principal function of the nose is to inhale air, removing noxious materials from the air stream, heating and humidifying inhaled air, protecting in this way the delicate distal pulmonary structures [1]. Furthermore, the nose itself produces a special gas called Nitric Oxide (NO) [2]. Nitric Oxide has several function:
Encouragement of ciliary motility, essential in trapping and removing dust and pathogens from the air [4].
Action as pulmonary vasodilator, that means reduction of pulmonary artery pressure and improvement of hemodynamic function [5].
Most normal breathing takes place through the nasal cavity, but the oral cavity (the mouth) can be used to supplement or replace the nasal cavity’s functions when needed. Unfortunately, the mouth does not warm and moisturize the air entering the lungs and it also lacks the hairs and sticky mucus that filter air passing through the nasal cavity, together with missing production of Nitric Oxide. So, if breathing through the nose is so powerful, why many people have necessity to mouth breathe?
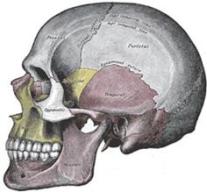
As a consequence of craniofacial development, the nasal airways are affected as well. Notice in Figure 2 the difference of a prehistoric skull against a modern one: the difference in the palate shape and airways size is massive. In modern days, we are assisting to a down-siding of the entire craniofacial structure, with the maxilla that drops down and back. This reduces the eye support, flattens the cheekbones, narrows the nasal airway, lengthens the mid facial third, and lowers the palate, which narrows and create malocclusion [6]. This also finds confirmation from the fact that expanding the maxillary arch results in an increase in airway dimensions [7,8,9,10].
Figure 2 – On the left, prehistoric skull: notice the large flat U-shaped palate and bigger airways. On the right, a modern skull with narrow high v-shaped palate and reduced airways. (From [11])If the nasal airways narrow, the nasal resistances increase and mouth breathe becomes a necessity, since easier[12,13,14]. If an inadequate craniofacial development can be seen as the cause of mouth breathing, in turn mouth breathing becomes the cause of an even worse craniofacial development. Indeed, when mouth breathing, the maxilla misses all the up and forward forces coming from the tongue and the teeth in contact: in this way, the maxilla remodels vertically and backward, developing malocclusion [15,16,17,18,19].
Have a look to Figure 3: the photograph on the left shows a boy at the age of ten. He breathes through his nose and he has a decently developed face, with defined eyes, cheekbones, lips and chin. When he was 14, he got a gerbil and developed an allergy that left him with a stuffy nose, which caused him to start breathing through his mouth. The photos in the middle and on the right show the same boy at the age of 17. Breathing through his mouth caused his face to grow downward instead of forward, making his face long and narrow.
Figure 3 – On the left, ten-year-old boy with decent facial development that was breathing through his nose. At the age of 14, he got a gerbil and developed an allergy that caused him to start breathing through his mouth. The photos in the middle and on the right show him at the age of 17: notice his complete different facial shape, with maxilla that grew vertically and backward. (From [40])The nose is well suited for breathing because it warms, humidifies and filters the air to prevent bacteria and particles entering the lungs. When nasal functions are impaired (i.e. when mouth breathing, when airways are narrowed or when septal deviations are present) airways are exposed to chronic irritation: this can result in enlarged adenoids and tonsils in children, easily obstructing the already narrowed nasal airways and further promoting mouth breathing [20]. Nasal function impairment is also linked to asthma and rhinitis [21,22,23,24,25,26,27].
And it does not end here. A vertical growth of the maxilla forces the mandible to swing back, restricting the pharynx (Figure 4). As compensatory mechanism, a retruded mandible causes the head to tilt forward in a forward head posture, freeing in this way the airways in the erect posture [28,29].
Figure 4 – Two patients from study [30]: subject HB003 shows vertical growth of maxilla, with facial retrognathism and large mandibular inclination. Notice the forward head posture and the reduced airways’ space. Subject HB092 shows forward growth of maxilla, with facial prognathism and small mandibular inclination. Notice the head posture aligned with the cervical column and the bigger space for the airways.
Restriction of the upper respiratory tract, including narrowing of both nasal cavity and pharinx, is a key element in the development of snoring and obstructive sleep apnoea [31,32,33]. When asleep, the compensatory mechanism of the head moving forward is missing: as shown in Figure 5, the mandible, the tongue and the soft palate obstruct the airways, causing either snoring or obstructive sleep apnoea, depending on the degree of obstruction. Interestingly, sleep apnoea has been associated to cardiovascular diseases and decline of cognitive functions [34,35,36].
Figure 5 – A forward-grown maxilla allows the mandible to be in a more forward position, creating no problems of airways obstruction during sleeping. A vertical growth of the maxilla forces the mandible to swing back. When sleeping the mandible, the tongue and the soft palate obstruct the airways causing either snoring or obstructive sleep apnoea. (From [41])
Also, a forward head posture requires the kyphotic curve to increase, with following increases of the lordotic curve and pelvic anteversion. An increased thoracic kyphotic angle is associated with a decline in inspiratory and vital capacity [37,38]. In addition, spinal deformation may result in a reduction in rib mobility and impairment of respiratory function. Spine misalignment may result in the loss of 30% of vital lung capacity, could be this one of the cause of many breathing disorders?
Breathing through the nose is essential for our body health. When it results difficult, the causes have to be searched into our craniofacial development. The implications of having breathing disorders are really detrimental for our body’s integrity, so do not underestimate them!
Snoring: is this noisy behavior just an embarrassing situation or is it a sign of an underlying problem? Why obstructive sleep apnea will almost always leads to loud and frequent snoring, while snoring does not always indicate sleep apnea? If you suffer of any of these two conditions, it is better that you understand where…