Over the last 50 years many theories have been put forward to explain the syndrome currently called Temporomandibular Disorders (TMD). However, it is doubtful whether any single theory fits all the complex features of this condition. The multifactorial explanation also appears flawed. So, what are the real underlying causes of this condition that exponentially spread over the last decades?
Many diseases do not have a clear-cut aetiology and this is especially true for temporomandibular disorders (TMD). Not only are there many competing theories to be considered, but a clear definition of the condition itself has yet to be agreed between the many disciplines involved in diagnosis and treatment. The term TMD usually refers to a cluster of disorders characterized by: pain in the preauricular area, the temporomandibular joint (TMJ), or the muscles of mastication; limitations or deviations in mandibular range of motion; noises in the TMJ during mandibular function [1]. Common other symptoms are jaw ache, earache and facial pain [2], with prevalence of migraine, tension‐type headaches and chronic daily headaches [3].
Despite this lack of consensus, clinicians are expected to provide care for TMD sufferers, especially if they are in pain, and a number of medical and dental treatment regimens have been developed. Even if patients see short term pain relief, a failure to establish the real etiology behind TMD leads many patients to fail responding to treatments over the long term. Patients often pass from one specialist to another, until they refuse further treatment or learn to accept their condition.
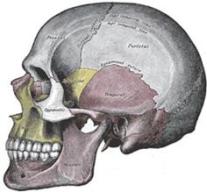
The term TMJ refers to the joints connecting the jawbone to the skull (Figure 1). A dense fibrous connective tissue, the articular disc, is positioned between the two bones forming the joint: the temporal bone and the mandible. The articular disc separates the condyle of the mandible from the articular fossa (also named mandibular or glenoid fossa) of the temporal bone.
Figure 1 – In the temporomandibular joint (TMJ), the articular disc divides the glenoid fossa of the temporal bone from the condyle of the mandible. (From [35])Lateral pterygoid muscle’s contraction pulls the disc and condyle forward within the glenoid fossa, leading to jaw opening. Three other muscles are responsible for closing the mouth (Figure 2): the masseter and the medial pterygoid muscles pull up the angle of the mandible, while the temporalis pulls up on the coronoid process of the mandible. The resting position of the mandible is determined by the teeth that when in contact stop the mandibular elevation.
Figure 2 – The lateral pterygoid muscle is responsible for opening the mouth, while the masseter, the medial pterygoid and the temporalis muscles are responsible to close it. (From [36])As mouth opens, the lateral pterygoid muscle pulls the disc and condyle forward, which then return to their resting position when the mouth closes (Figure 3). The normal resting position of the condyle is in the middle of the glenoid fossa. In cases where this centric relation is missing, the condyle can move too far back (condylar displacement), squeezing the disc out of the way. This is known as disc displacement [4] and it can cause clicking and locking of the TMJ:
In clicking jaws, as mouth opens, the disc is pushed anteriorly until a click occurs, at which time the disc returns to a normal relationship with the condyle. During the closing movement, the disc is again displaced anteriorly [5].
In close-lock, the condyle is blocked behind the anterior displaced disc, with limited mouth range of motion during opening [6,7]. In open-lock, the condyle is entrapped in front of the lagging disc and cannot slide back under the fossa, with difficulty in mouth closure [8].
Figure 3 – In a normal TMJ, the condyle and the disc move together. In clicking and locking, the disc is displaced, causing a click if the condyle returns in normal relationship with the disc during mouth motions, or a lock if the condyle is not able to return in a normal relationship with the disc. (From [37])The central area of the articular disc is avascularised and lacks of sensory innervation, while the peripheral region has both blood vessels and nerves. In cases of posterior condyle displacement, the condyle moves too far back, pinching the innervated tissue with resulting pain. This is further exacerbated in case of disc displacement, since the condyle directly compresses the vascular and innervated area of connective tissue against the articular surface of the temporal bone (Figure 4).
Figure 4 – On the left, normal resting position. On the right, case of disc displacement in which the condyle compresses the vascular and innervated area of the connective tissue, causing pain. (From [38])
The most common treatment for TMD is splint therapy, consisting in wearing intra-oral dental appliances with occlusal coverage (a more or less thick layer over the teeth) [9]. But is splint therapy a valid treatment for TMD? Over the short term, it provides pain relief, but it does not treat the underlying cause of TMD: splint therapy is just a good way to treat the symptoms, but not the causes. Let us explain better how.
A splint is usually a few-millimeter-thick device, inserted between the teeth. This layer induces the mouth to stay in a sort of open-mouth posture, with the condyle moving forward in a possible centric relation, being also able to catch the disc if displaced. In this way, the connective tissue is not compressed and the patient is pain free (Figure 5). Also, the muscles responsible for mouth closure, i.e. the masseter and temporalis muscles, lengthen and relax, giving relief from muscle pain [10].
Figure 5 – A splint of few millimeters between the teeth rest the mouth into an open-mouth posture, with the condyle that move foward catching an eventual displaced disc. In this way the patient is pain free. (From [39])Although a splint may provide almost instant pain relief, many clinicians lack the knowledge of the consequences of using it. Indeed, the body is a very dynamic system and a splint in the mouth brings its drawbacks over the long term. First of all, bones remodel continuously in our body and so do bones in the TMJ, which are very adaptive: indeed, both condyle and glenoid fossa remodel very quickly to accomodate the new forward position [11,12], as Figure 6 shows.
Figure 6 – Young adult girl aged 16 years 1 month before Herbst treatment. She is in skeletal maturity stage. Intraoral photographs, MRIs of both left and right TMJ and corresponding tracings of TMJ area from different treatment stages are shown: before treatment (T0), at start of treatment (T1), at 12 weeks of treatment (T2) and after treatment (T3). Outline of condyle and glenoid fossa and appositional areas are marked in tracings. (From [11])And here comes the first drawback. When closing the mouth, the teeth determine the resting position of the mandible. But if the glenoid fossa and the condyle remodeled into a new forward position and the teeth did not change, what happens when the splint is removed? The condyle moves further back in the fossa, worsening the TMD. To solve this, teeth should erupt to accomodate the new mandibular position and maintain the contact between upper and lower arches. However, a further problem arises: teeth not in contact extrude, while when in contact they intrude [13]. So, when wearing the splint, teeth are in contact with it and they do exactly the opposite of what is needed: they intrude [15]. In this way, when removing the splint, the mandible moves further back, further worsening the TMD.
It is clear that there is a real need to find the causes of TMD to be able to find an appropriate therapy treating the cause and not the symptoms. So, what are the causes of TMD? A poor craniofacial development! Indeed, the mandibular position directly depends on the development of the maxilla. In recent days, we are assisting to a down-siding of the entire craniofacial structure, with the maxilla that drops down and back. This reduces the eye support, flattens the cheekbones, narrows the nasal airway, lengthens the mid facial third, and lowers the palate, which narrows and create malocclusion [15]. If the maxilla grows vertically, the mandible swings back giving predisposition of TMD (Figure 7) [16].
Figure 7 – In a forward grown maxilla, the mandible is able to move in a more forward position (on the left). If the maxilla grows vertically, the mandible is pushed back, giving predisposition of TMD (on the right). (From [40])Forces remodeling the maxilla come from the tongue and the teeth (through the masseter muscles), so splints have another problem: by relaxing and lengthening the masseter muscle, the maxilla further remodel vertically. This also worsens TMD. Also, an upper splint can remove space for the tongue, hitting its normal resting posture on the roof of the mouth.
People with open-mouth posture, that include mouth breather, are those with higher risks of developing TMD. Indeed open-mouth posture is a common sign of TMD, together with retroposed condyles, tongue between tooth posture, occlusal irregularities, lingual inclination of the teeth, and deformation of the condyle and fossa [17].
Joints are highly adaptable and will always remodel to suit habitual rest positions. This is confirmed by patients with anterior disc displacement that have a natural reduction of the symptoms after some time [18,19]. But, if the mouth is continuously held open, the temporomandibular joint will recontour so that the head is maintained near the centre of the fossa when in that position. When the mouth is then closed, the head of the condyle moves upwards and backwards, occupying a position frequently seen in TMD cases (Figure 8) [20,21].
Figure 8 – In an open-mouth posture, the condyle and the glenoid fossa remodels to suit the habitual resting position. When the mouth is closed, the condyle moves upwards and backwards, causing pain. (From [41])Cranial distortions are another important factor in the etiology of TMD. As Figure 9 shows in the case of left side bending, the mandibular condyle follows the temporal bone causing the entire mandible to rotate around to the left and back. The maxilla instead rotates to the exact opposite direction, giving predisposition of one condylar disc to be anteriorly displaced (the one on the left in case of left sidebending) and the other posteriorly displaced (on the right in left sidebending) [22]: internal derangement of TMJ is a common feature of patients with facial asymmetry [23,24,25].
Figure 9 – Relation of cranial base with maxilla and mandible in case of left sidebending. Occipital bone and mandible are sketched with the same red colour since they relate each other, while maxilla and sphenoid are in blue. This asymmetry gives predisposition to internal derangement of TMJ. (From [22])Our body is a complex but perfect system, with many inputs and outputs. The posture is an output of this system, with inputs coming from vestibular, visual and somatosensory systems [26,27]. The trigeminal nerve is the largest of the cranial nerves and provides important inputs for the postural control (Figure 10). It is composed by three branches connected to the eyes (visual input), the maxilla and the mandible (somatosensory inputs). Another branch reaches the ear, where the vestibular system is present (vestibular input). This nerve feeds the brain with information related to balance, the horizon, verticality and the position of the skull with respect to the mandible and the body. This is why TMD is usually related with postural imbalance [28,29,30]
Figure 10 – The trigeminal nerve has three major branches connected to the eyes, the maxilla and the mandible. It is one input of the somatosensory system for postural control. (From [42])Also, in many cases of TMJ internal derangement, the auriculotemporal nerve (a small branch of the mandibular nerve) can become drawn into the compression zone of the TMJ, with possible neuroinflammation. This neuroinflammation may spread and can act as physiological driver for aberrant reflexive behaviors, arising movement disorders, e.g. dystonia, Tourette’s syndrome [31,32]. As TMJ is in a direct relationship with the cranial structure and body posture, TMD is also linked with many disorders associated with poor body posture and craniofacial development, such as fibromyalgia [33] and multiple sclerosis [34].
In brief, TMJ is a very adaptive and dynamic joint and it is the most used in the body. TMD is currently poorly understood because many treatments involve splints, only relieving the symptoms and ignoring the real causes. The underlying issue depends on the craniofacial development, reason why TMD is then linked to many other disorders.
One thought on “Temporomandibular Joint Dysfunction (TMD)”
I had the same urge to write articles about my journey to treat TMD but am 10 degrees of pain away from actually doing so. Sorry about your experience but thank it for delivering this blog.
I also wore a splint, for 2 years and only at night. It unlocked my TMJ and eased symptoms overall. I have no pain right now but clicking is still present. My doctor (from China) also were too stubborn to follow guidelines on their sociopsychological model. He digs into jaw relationship and muscles, while not ignoring teeth. I think you’ll find his articles useful.











I had the same urge to write articles about my journey to treat TMD but am 10 degrees of pain away from actually doing so. Sorry about your experience but thank it for delivering this blog.
I also wore a splint, for 2 years and only at night. It unlocked my TMJ and eased symptoms overall. I have no pain right now but clicking is still present. My doctor (from China) also were too stubborn to follow guidelines on their sociopsychological model. He digs into jaw relationship and muscles, while not ignoring teeth. I think you’ll find his articles useful.
https://www.sciencedirect.com/science/article/pii/S0208521623000797
https://mp.weixin.qq.com/s/SxJKP4qj6KfJM8oOt6wRow
LikeLike