The tongue: not many people truly understand the importance of this muscle for body’s health, with the consequence of unconsciously establishing wrong habits in newborns that persists for the rest of their life. Malocclusion and many diseases exponentially spread with civilization: the causes have to be found in many acts of modern lifestyle that affect tongue posture and function.
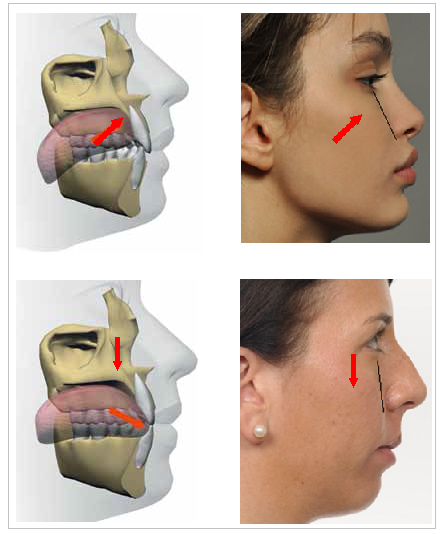
As highlighted in Figure 1, maxilla is primarily remodeled by forces coming from tongue and teeth (through masseter muscles). When these forces are missing, the maxilla drops down and backwards. This reduces the eye support, flattens the cheekbones, narrows the nasal airway, lengthens the mid facial third, and lowers the palate, which narrows and creates malocclusion [1]. Thus, malocclusion is just a consequence of the craniofacial development.
Figure 1 – Tongue posture directly affects maxilla remodeling. When the tongue is correctly on the roof of the mouth, maxilla is remodeled up and forward (above case). Instead, when the tongue is not in the correct position, maxilla misses its forces and remodels down and backwards (bottom case). Notice the difference in cheekbones, eyes support, nose shape, length of the face and lips shape. (Adapted from [37] and [38]).
The causes of malocclusion and of poor craniofacial development have to be found in the modern lifestyle, in particular in:
Increasing of bottle-feeding over breast-feeding that influences the swallowing pattern and all oral muscles [2,3,4,5].
Use of the pacifiers/dummies that mainly affects tongue posture [6,7,8,9].
Trend towards industrial soft high-calorie food that hits chewing effort and muscles action [10,11,12].
Trend towards an earlier or too early weaning, influencing swallowing pattern [13,14].
A poor craniofacial development has also direct consequences on breathing: when nasal airways narrow, air resistance through the nose increases and mouth breathe becomes a necessity, since easier [15,16,17]. This further worsens the craniofacial development and gives predisposition of allergies, nasal congestion, enlarged adenoids and tonsils that further promote mouth breathing [18,19,20,21,22,23].
Figure 2 shows the consequences of using artificial nipples and pacifiers/dummies in newborns. The tongue posture is low, the mouth is open: this becomes a habit that will persist for all the life of the individual, affecting his craniofacial development. This is why open-mouth habits do not necessarily coincide only with mouth breathing [24].
Figure 2 – Using artificial nipples and pacifiers/dummies in newborns has the consequence of creating a low tongue posture and mouth open that will persist for all the life of the individual, affecting his craniofacial development. (From [39])
With a pacifier, the newborn learns to swallow with an open-mouth and low tongue posture. Then, this type of swallow becomes a habit and, growing up, children continue to swallow with their jaws apart: the teeth are not placed in occlusion and the tongue is thrust between the dental arches, creating open bite malocclusion (Figure 3).
Figure 3 – Tongue thrusting is the habit of having the tongue between the teeth before and during the act of swallowing. This causes an open bite malocclusion. (From [40])
Many dentists and orthodontists believe that the shape influences the function. Applied to the mouth, this means open bite malocclusion (which is labelled with unknown or genetic etiology) would cause tongue thrust. Although over the short term this is true, they forget that over the long term teeth and bones remodel with light-mid forces, meaning that it is actually tongue thrusting (the function) that creates malocclusion (the shape) [25]. Otherwise, why correcting the tongue posture would also correct the malocclusion (see the work of John Mew and Orthotropics, Figure 4), while by only correcting malocclusion (with traditional braces used in Orthodontics) the final result relapses [26]?
Figure 4 – Underdeveloped jaw of Charlotte. She was waiting for surgery, but she has been successfully treated with Orthotropics, obtaining remarkably facial changes.
The tongue is a very mobile and strong muscular organ capable of undergoing great changes in length and width at every contraction of its muscles, exercising great pressure. The importance of its function are understood only by few people, reason why its role is often neglected.
Another often misunderstood condition is tongue-tie (Figure 5). In newborns, the tip of the tongue is as yet incompletely developed, with the frenulum extending almost to the tip. During the early weeks of life, the tongue grows longer and thinner, the frenulum stretches and its tongue attachment recedes [27,28]. There is no literature confirming this, but there are many clues suggesting that, with bottle-feeding and pacifiers, the frenulum cannot stretch properly since the tongue has a low posture and function, creating in this way the tongue-tie.
Figure 5 – Tongue tie is a misunderstood condition. In the presence of bottle-feeding and pacifiers, tongue function is altered. Then, the function affects the form, with predisposition to tongue-tie. (From [41])
Tongue-tie leads to breast-feeding difficulties, leaving many mothers with the necessity to bottle-feed their babies [29]. However, breast-feeding and bottle-feeding have two completely different mechanisms:
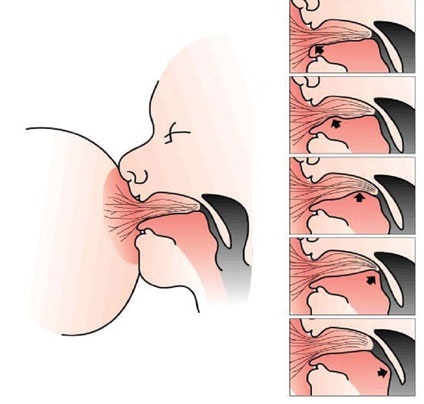
In breast-feeding (Figure 6), the nipple and part of the surrounding areolar tissue are drawn into infant’s mouth, which extends the tongue over the lower gum pad. The lips are responsible to create a good seal with the areolar tissue. Initial suction is required to extend the mother’s breast and nipple into the hard and soft palate. As long as the seal remains intact, no further suction is required. To start the milk flow, the infant must compress the mother’s lactiferous sinuses located in the areolar tissue and, with a peristaltic (rolling-like) action of the tongue that compresses the nipple against the palate, the milk moves toward the throat. This swallowing pattern sets a habit maintained into adulthood for the correct swallow [30,31,32]. Furthermore, when not sucking or swallowing, babies rest the tongue indenting the nipple (the famous tongue on the roof of the mouth posture) [32].
When bottle-feeding, the lips seal is not strictly required (open-mouth posture) and the milk needs a greater sucking action to flow, meaning the tongue acts with a squeezing (piston-like) motion [32], a complete different motion with respect to breast-feeding. Artificial nipples with a big hole force the baby to hold the tongue against the nipple to stop the abundant flow of milk from the bottle. This is exactly how tongue-thrust originates. Furthermore, when not sucking or swallowing, bottle-fed babies rest with the latex-teat expanded (low tongue posture) [32,33,34].
Figure 6 – During breast-feeding, sucking action is required only to bring the nipple into the hard and soft palate. Lips are responsible to create a good seal and, as long as the seal is preserved, no further sucking is required. The milk is then obtained with a peristaltic motion of the tongue, which compresses the nipple against the hard palate moving the milk toward the throat. This pattern set the correct normal swallow into adulthood. (From [30])
When mothers are concerned about the influence that bottle-feeding and pacifiers may have on dentition, many practitioners say that they are not harmful until the first permanent teeth come out. But this is absolutely wrong! Bottle-feeding and breast-feeding require two completely different function and posture of the tongue. Then, these two factors have a tremendous impact on the craniofacial development and, thus, malocclusion [35,36].
There are many misconceptions in the current medical world, with practitioners unable to understand the importance of certain newborns’ actions. Craniofacial development mostly depends on tongue function and posture and it is essential for future health of the individual. From TMD to multiple sclerosis, from hair loss to Alzheimer, this website collects the clues that link many disorders to a poor craniofacial development. Future health of an individual depends from the very first days of his life, so do not neglect your actions towards newborns!
In life nothing is guaranteed, there are many aspects to take into account. Bone remodeling is greater in earlier years of life, so “reversing” is not really an appropriate term. However, it is my believe you can see notable changes.





possible to reverse CFD if not so young? I am willing to put in the work provided im guaranteed results
LikeLike
In life nothing is guaranteed, there are many aspects to take into account. Bone remodeling is greater in earlier years of life, so “reversing” is not really an appropriate term. However, it is my believe you can see notable changes.
LikeLike