When it comes to palatal expansion, many options are available that can sometimes create confusion for us patients. The confusion comes from the use of very similar names/acronyms and procedures that can seem very similar, which however carry substantial differences. Hopefully this article can clarify what are the options available and the differences between them.
The fist distinction to have in mind is the one between tooth-borne, bone-borne and hybrid expanders:
- Tooth-borne expander: tooth-anchored device that transmits its expansion forces through the supporting teeth.
- Bone-borne expander: these devices are directly attached to the palate by means of mini-screws, with forces applied directly to the maxilla.
- Hybrid expander: the combination of a tooth-borne and bone-borne appliance, with anchorages on both the teeth and the palate.
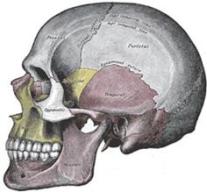
The maxilla is the upper paired bone of the jaw, with the two maxillae that unite with each other at the intermaxillary suture. It has four processes: zygomatic, frontal, alveolar and palatine process.
- The zygomatic process is the extension of the maxilla that articulates with the zygomatic bone by means of the zygomaticomaxillary suture.
- The frontal process is a strong vertical plate that forms part of the lateral boundary of the nose as well as the medial border of the orbit. It connects with the nasal bone, frontal bone and other bones.
- The alveolar process is the thickest part of the maxilla that contains the tooth sockets.
- The palatine process is a horizontal extension of the maxilla that constitutes the roof of the mouth and the floor of the nasal cavity. Together with the palatine bone it forms the hard palate. The palatine bone posteriorly articulates with the sphenoid bone, which main function is to provide the foramina and canals for the passage of neurovascular structures to and from the cranium.

Although we might think that an expander has only a direct effect on the palate and the teeth, the reality is that the human body is a fairly complex system, where things cannot be seen in isolation. It is thus essential to understand the craniofacial complex in its entirety. For example, the zygomatic bone articulates with the maxilla, the temporal bone, the sphenoid bone and the frontal bone. It should be easy to understand that any force applied to the maxilla will also affect the zygoma, which also affect the sphenoid bone and so on. Similarly, the palate is constituted by the palatine process of the maxilla for three quarters, while one quarter is composed by the horizontal plate of the palatine bone. Any expansion in the palate will thus affect the palatine bone, which will have repercussion on the sphenoid bone.
Since everything in the human body is connected, the development of the craniofacial complex has repercussion on the whole body. While many patients seeking palatal expansion are primarily concerned about their Obstructive Sleep Apnea (OSA), breathing problems or smile, it is important not to overlook other important consequences of these procedures. For example, posture is one of the main consequences of craniofacial development. Unfortunately, the reality is that many orthodontists and dentists neglect the need to look at the body in a holistic way and thus neglect the possible consequences that a palatal expansion can have on the holistic health of an individual. Given that the scope of this article is to shed some light on the different palatal expansion procedures, we will not cover the possible consequences that this can have on the whole human body. But please be aware! This website is full of resources in this sense, so do not stop here in your research of knowledge.
RPE (Rapid Palatal Expander), RME (Rapid Maxillary Expander)
RPE (Rapid Palatal Expander) or RME (Rapid Maxillary Expander) is the least invasive expansion technique which uses tooth-borne expanders to widen the upper jaw. The device is placed in the roof of the mouth and anchored to the teeth, resulting in forces applied directly to the teeth. The expansion is achieved by turning the screw (the most popular type is the Hyrax screw), which is generally placed in the middle of the appliance. The forces will result in opening of the palatal suture and new bone being formed in the palate. While this is effective for skeletal changes in patients at a young age which can opt for a rapid (one turn of the screw per day) or slow expansion (at a more physiological rate of 1 turn every other day), it can lead to more dental than skeletal changes for older patients, with possible excessive tipping of the teeth and other complications.

MARPE (Miniscrew-Assisted RPE), MSE (Maxillary Skeletal Expansion), EASE (Endoscopically-Assisted Surgical Expansion)
According to some studies, the midpalatal suture begins to obliterate during the juvenile period, and the ossification of both the midpalatal suture and circummaxillary sutures increases with age. The increase in the degree of suture fusion makes it difficult to expand the maxilla in older patients, with also possible undesired side effects like excessive dento-alveolar tipping, root resorption and periodontal damage in the form of gingival recession or fenestration of the buccal bone of supporting teeth. To minimize these side effects and to avoid surgical methods like SARPE, MARPE/MSE is generally preferred for palatal expansion in adult patients.
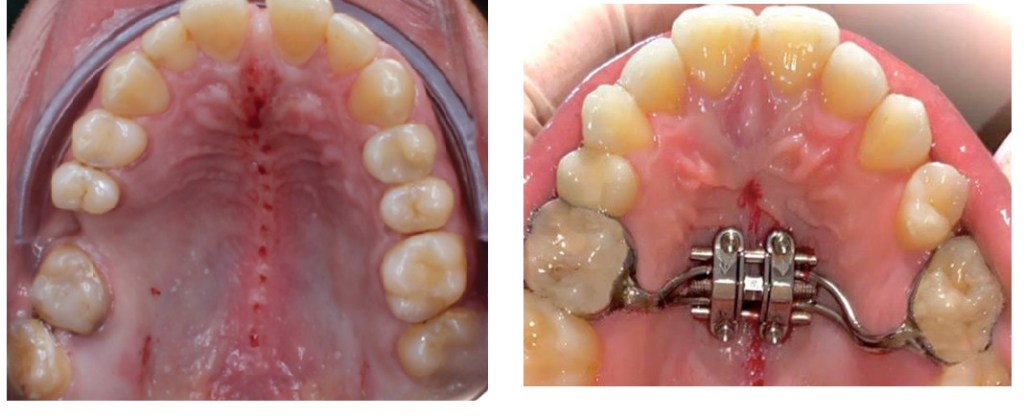
MARPE (Mini-screw or Mini-implant Assisted Rapid Palatal Expansion), also known as MSE (Maxillary Skeletal Expansion) is an appliance positioned and anchored directly on the maxillary bone, bringing horizontal expansion forces close to the midpalatal suture. There are different variations of the appliance, some with connecting arms attached to the teeth, others without teeth anchorage. When the teeth anchorage is present, the appliance is referred to as hybrid or tooth-bone-borne appliance. Studies have shown that arms prevent the distal rotation of the teeth when the appliance is activated.
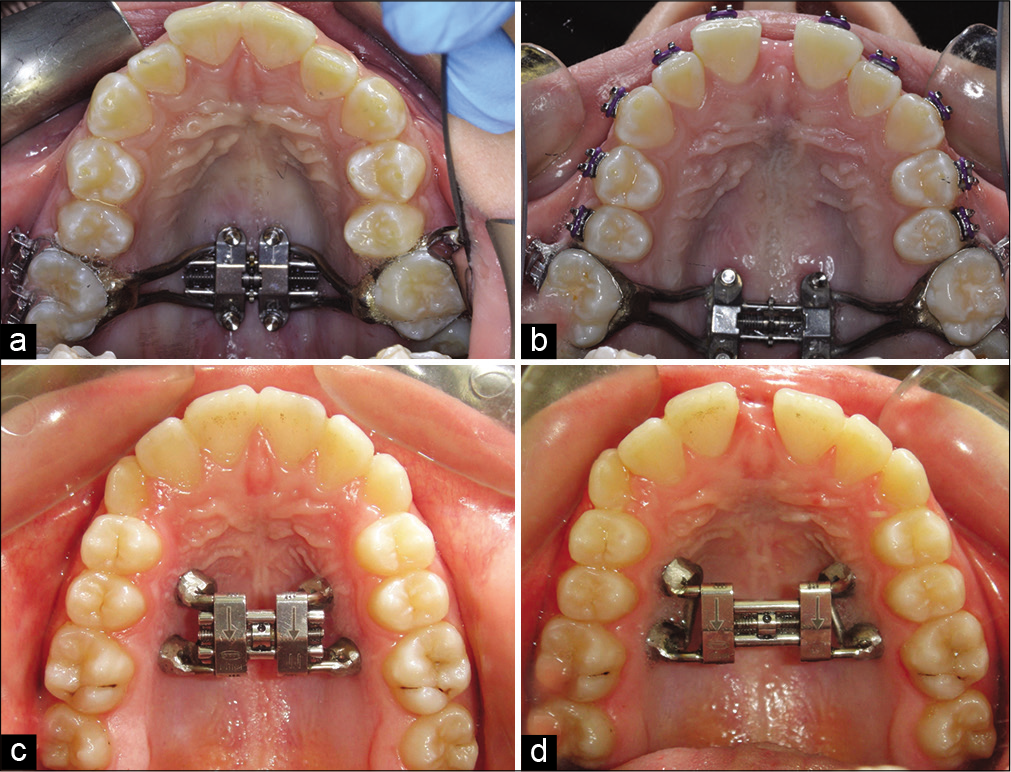
Bone-borne palatal expansion relies on skeletal anchorage obtained through mini-implants to directly apply forces to the maxilla, close to the midpalatal suture. The effectiveness of the expansion thus depends also on the stability of the mini-implants, which directly affects the stability of the appliance. These mini-implants are also referred as Temporary Anchorage Devices (TADs).
Different anatomical factors come into play for the stability of the mini-screws:
- Bone depth.
- Cortical bone thickness.
- Bone density.
- Soft tissue thickness.
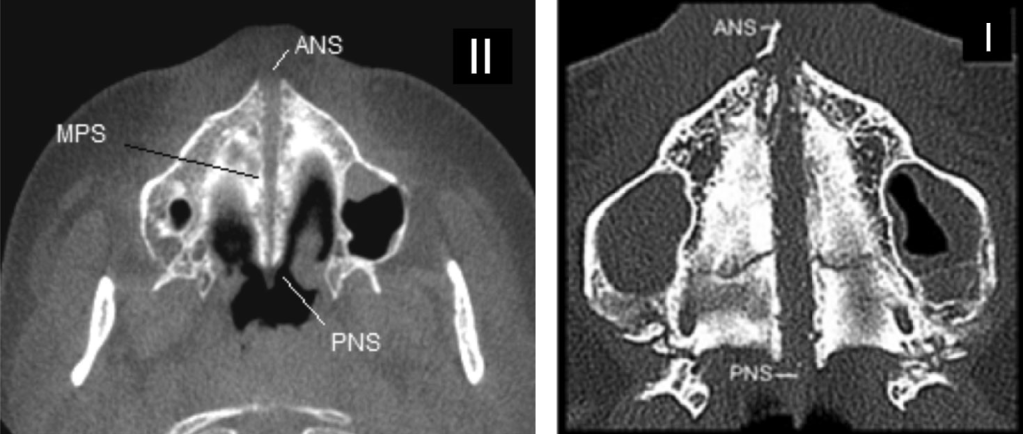
The below picture shows the division of the three parts of the palate: the anterior segment before the incisive foramen; the middle segment from the incisive foramen to the transverse palatine suture; the posterior segment, after the suture to the palatal bone.
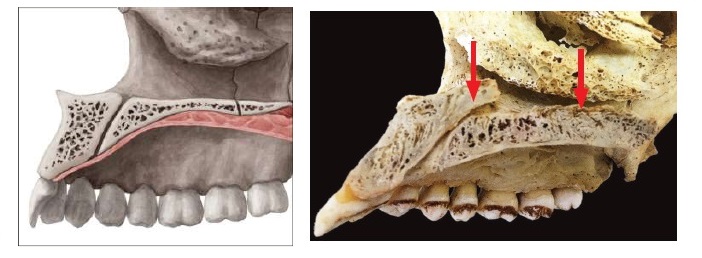
Different studies have analyzed the bone density of the palate, showing that:
- The midpalatal area close to the midpalatal suture has the thickest bone.
- The further posterior part of the palate presents lower bone density (as can be also seen from the picture above).
- Male individuals have generally higher bone density.
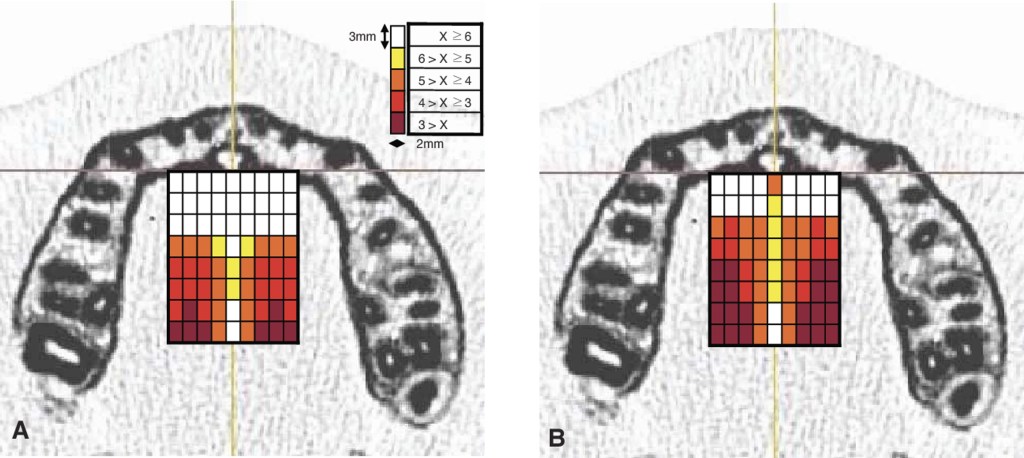
Thicker bone represents a better anchorage for the screws, reducing the risk of screw dragging. For this reason, doctors prefer to place the appliance more anteriorly in the midpalatal segment to reduce the risks of failure. The anterior segment also presents less resistance from other surrounding structures, thus more anteriorly the appliance is placed, more expansion can be achieved in the anterior segment. However, the posterior part has a higher resistance, because it is more engaged with other surrounding structures (for example think about the engagement of the zygomatic area, palatine and sphenoid bone that happens more posteriorly). This can thus result in a more conical/triangular or V-shaped expansion, which implies less benefits for the expansion of the airways (less nasal volume increase) and less midface changes.
An appliance placed more posteriorly increases the chances of a more parallel expansion of the midpalatal suture, thus resulting in more benefits for the nasal volume and midface. However, this presents also higher risks of failure since the resistance in that area of the palate is higher and the bone is less dense. The forces generated by the appliance have to overcome the resistance located in the midface such as the pyriform aperture pillars, zygomatic buttresses, pterygoid junctions, midpalatal suture, etc.
While higher bone density increases with age and can represent a good anchorage for the screw, older patients might also present increased sutural bone density of the midpalatal suture, reduced bone elasticity and higher fusion of the circummaxillary sutures, which overall means higher resistance for the appliance. Research has been conducted in order to find minimally invasive procedures that can facilitate palatal expansion, reducing the resistance of surrounding structures. For example, while studies on skeletal expansion have shown that pterygopalatine suture can be split with the expansion itself, supportive surgery might be preferred by doctors to obtain pterygopalatomaxillary separation and thus reducing the chances of failure. This is similar to what is achieved with the EASE procedure. Other studies aimed at finding ways of reducing the resistance of the midpalatal suture, identifying surgical methods like corticotomy, microperforations, piezocision, corticopuncture and corticision to perform perforation of the midpalatal suture.
Bone density also plays a role in determining the type of anchorage for the miniscrews, aiding choosing between monocortical (perforation of the palatal cortical bone only) and bicortical (perforation of both the palatal and nasal cortical bone) insertion. When the monocortical insertion of miniscrews is used in individuals with thick suture or with great resistance to maxillary separation, distortions or folds may occur in the Temporary Anchorage Device during activation of the expanding screw. Bicortical insertion is recommended in these cases. Certain studies have also shown that bicortical insertion leads to higher skeletal expansion versus dental expansion when compared to monocortical.

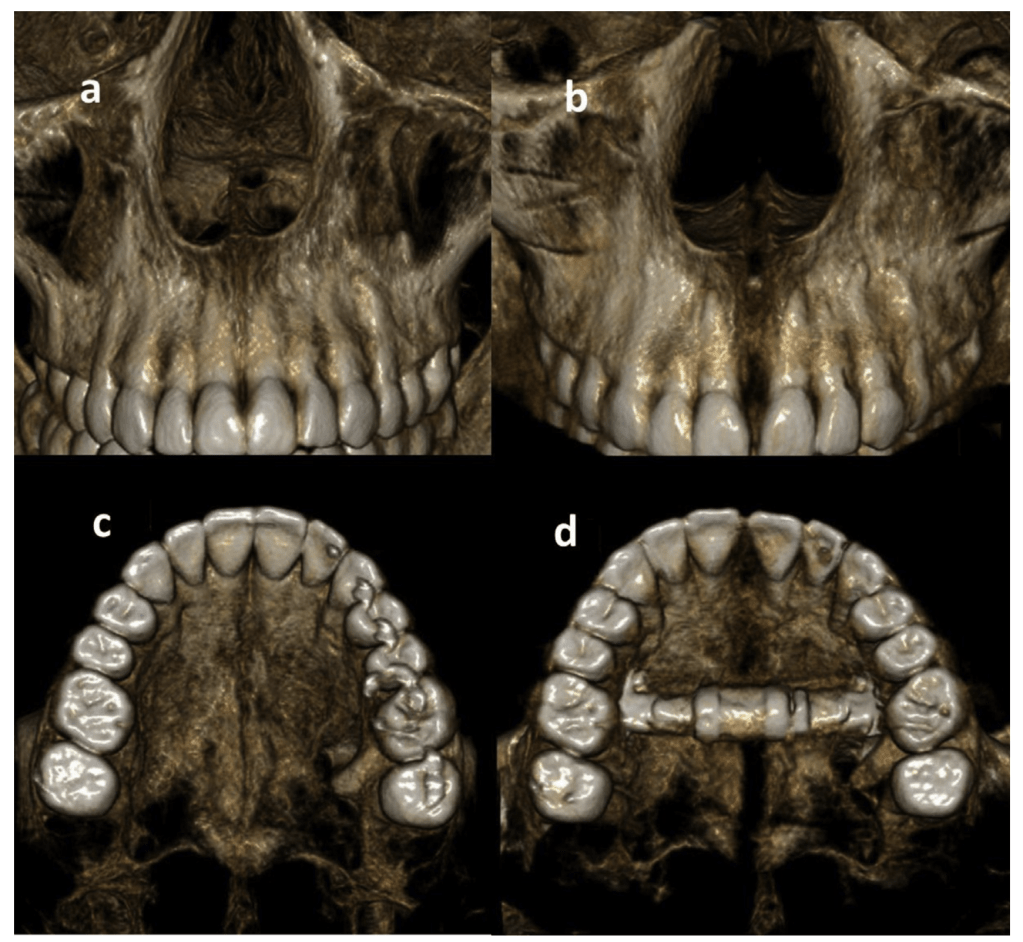
The usual protocol of expansion for MARPE consists of turning the expansion screw twice per day until a diastema is formed between the incisor teeth. The diastema is the clear sign that the midpalatal suture has split. After that, the expansion is progressed with one turn per day. Other protocols have also gained popularity, although studies are missing to compare the different methods. One protocol consists of alternating expansion/activation periods with constriction periods. The rationale for this protocol is that it weakens the circummaxillary sutures, resulting in higher mobilization of the sutures and weakened resistance structures (like the sphenoid). Some studies have also shown that this could aid forward movement of the maxilla by means of facemask therapy, although not enough literature is present to validate this claim.
Some studies have suggested the pterygomaxillary junction as the point with the highest resistance during expansion. This resistance influences the expansion with possible failures or a V-shaped expansion. A V-shaped expansion reduces the benefits for patients seeking ways to correct their airways problems, with a reduced expansion of the nasal volume. For this reason, Dr. Kasey Li developed a procedure called EASE (Endoscopically-Assisted Surgical Expansion).
While literature on the procedure is missing, the common understanding is that EASE sits in between MARPE and SARPE. A transpalatal distractor (TPD) with footplates stabilized with a screw is placed in the palate and the expansion is facilitated by achieving pterygomaxillary separation with a piezoelectric blade. A midpalatal osteotomy is also performed to reduce the midpalatal suture resistance. The result is a more parallel expansion of the midpalatal suture, increased nasal volume and reduced diastema.

One of the well-known problems of MARPE is asymmetrical expansion, which can have a repercussion on the whole body. EASE should provide higher chances of symmetrical expansion due to the disengagement of the pterygomaxillary sutures.
SARPE (Surgically-Assisted RPE), DOME (Distraction Osteogenesis Maxillary Expansion)
SARPE (Surgically-Assisted Rapid Palatal Expansion), also known as DOME (Distraction Osteogenesis Maxillary Expansion), is a combination of both Oral and Maxillofacial Surgery and Orthodontics that is done to achieve a more predictable maxillary skeletal expansion in adults. It combines a maxillary expander anchored to the palate by mini-implants with minimally invasive LeFort I osteotomies. Midpalatal osteotomy is also performed to break the inter-maxillary suture. Usually, the pterygoid plates are not involved in this procedure. However certain surgeon might decide to separate the plates. The separation is called pterygomaxillary disjunction, PMD.

SARPE procedure results in palatal expansion as well as nasal volume increase. The chances of failure are reduced due to the various osteotomies. Exactly for this reason however, the engagement with other sutures and bones is missing, resulting in less changes in the midface. Chances of asymmetrical expansions are also lower.
Final Considerations
Palatal expansion can be achieved by means of different methods. While RPE is usually indicated for the pediatric patients, more invasive treatments are necessary for adult patients. MARPE offers a good compromise in terms of the necessary forces to split the midpalatal sutures, without invasive osteotomies. Several studies have shown success rate of MARPE being greater in female vs male (generally due to bone density), with increased chances of failure as the age increases. Corticotomy is sometimes used to aid palatal suture split. Given the engagement of surrounding structures with MARPE, the appliance must overcome higher forces. This can result in higher chances of failures and asymmetries, especially in the case of patients with already-existing asymmetries, since one side shows greater resistance than the other.
SARPE reduces the engagement of the surrounding structures, thus resulting in reduced chances of failures, as well as reduced chances of asymmetrical expansions. The expansion of the midpalatal suture is more parallel, resulting in higher increase of the nasal volume. However, higher the disengagement of the surrounding structures, less changes are achieved in the midface, including the zygoma.
A more posterior MARPE generally allows a more parallel expansion of the midpalatal suture, but this can result in higher chances of failure due to the lower bone density of the posterior part of the palate.
One thing to consider is that even minimally invasive procedures like the corticotomy of the midpalatal suture carry their own risk. More invasive the procedure, higher the chances of complications. The research of an experienced and well-trained practitioner is thus essential.
Any expansion needs retention as otherwise the tendency is for the body to return to its initial state. Usually, retention is recommended for 1 year after expansion to allow full bone remodeling. A transpalatal arch is not enough to avoid bony relapse, TADs are needed.
Different expansions protocols are present. Slow expansion can still achieve sutural opening and it is also more physiological, with smaller diastemas. Other protocols alternate expansion with retraction, aiming at reducing resistance at the sutures. However not enough literature is present to better understand its effects.
Unfortunately, not many doctors understand the consequences of a palatal expansion in the holistic view of the body, for example, how asymmetries can lead to body torsions, with scoliotic tendencies. We can only hope that some doctors will realize the consequences of certain procedures and thus will explore the studies of the human body in a holistic manner.

This is the only article I can find that explains the difference between these procedures so clearly, from a patient perspective. Thanks so much for writing these. As patients, it is very difficult to navigate through TMJ/Airway problems as every practitioner has its different procedures.
LikeLike
I’m glad this was helpful!
LikeLike
Hi! nice article! do you have information of M.I.N.D technique?
LikeLike
Can you make an updated article including FME and its’ face mask FMA?
LikeLike